Potrebbero piacerti anche
- Jurnal 4Documento9 pagineJurnal 4Tia AriantiNessuna valutazione finora
- Daftar PustakaDocumento1 paginaDaftar PustakaTia AriantiNessuna valutazione finora
- Brosur Penyuluhan Gizi Anak SekolahDocumento2 pagineBrosur Penyuluhan Gizi Anak SekolahTia AriantiNessuna valutazione finora
- Aturan Minum FitbellyDocumento1 paginaAturan Minum FitbellyTia AriantiNessuna valutazione finora
- Jurnal 4Documento9 pagineJurnal 4Tia AriantiNessuna valutazione finora
- Jurnal 1Documento13 pagineJurnal 1Tia AriantiNessuna valutazione finora
- The Effect of Carvedilol On Morbidity and Mortality in Patients With Heart FaliureDocumento7 pagineThe Effect of Carvedilol On Morbidity and Mortality in Patients With Heart Faliurecobby174Nessuna valutazione finora
- Jurnal 3Documento10 pagineJurnal 3Tia AriantiNessuna valutazione finora
- Penyakit Jantung HipertensiDocumento24 paginePenyakit Jantung HipertensiTia AriantiNessuna valutazione finora
- 12-Lead EKG Analysis Fall 20021Documento48 pagine12-Lead EKG Analysis Fall 20021Yesi SaputriNessuna valutazione finora
- Falciparum Malaria by DR SarmaDocumento65 pagineFalciparum Malaria by DR SarmaTia AriantiNessuna valutazione finora
- Demam 2Documento30 pagineDemam 2Tia AriantiNessuna valutazione finora
- Aids KulDocumento71 pagineAids KulTia AriantiNessuna valutazione finora
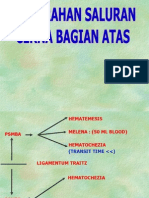
- Perdarahan Saluran Cerna Atas Dan BawahDocumento24 paginePerdarahan Saluran Cerna Atas Dan BawahTia AriantiNessuna valutazione finora
- 2014 ESC Management of Antithrombotic Therapy in Atrial Fibrillation 1Documento25 pagine2014 ESC Management of Antithrombotic Therapy in Atrial Fibrillation 1Tia AriantiNessuna valutazione finora
- Diabetes Mellitus - Kuliah2013Documento190 pagineDiabetes Mellitus - Kuliah2013Tia AriantiNessuna valutazione finora
- Demam Tifoid. KulDocumento60 pagineDemam Tifoid. KulTia AriantiNessuna valutazione finora
- Soal Ujian EkgDocumento12 pagineSoal Ujian EkgTia AriantiNessuna valutazione finora
- EKG BacaDocumento59 pagineEKG BacaTia AriantiNessuna valutazione finora
- PedNas TB 2011-Isi A PDFDocumento59 paginePedNas TB 2011-Isi A PDFYesi SaputriNessuna valutazione finora
- 09 Diuretics Upd 2Documento42 pagine09 Diuretics Upd 2Ritari KimyunjongNessuna valutazione finora
- Hepatic EncephalopathyDocumento16 pagineHepatic EncephalopathyTia AriantiNessuna valutazione finora
- Hepatitis (DR - Lukmanhakim Usu)Documento36 pagineHepatitis (DR - Lukmanhakim Usu)Tia AriantiNessuna valutazione finora
- KOLELITIASIS1Documento37 pagineKOLELITIASIS1Tia AriantiNessuna valutazione finora
- Fatty Liver - HandoutDocumento31 pagineFatty Liver - HandoutTia AriantiNessuna valutazione finora
- RLCirrhosisPortal HTNMunireddy0207Documento41 pagineRLCirrhosisPortal HTNMunireddy0207Tia AriantiNessuna valutazione finora
- Congestive Heart Failure CHF: Nik Nikam, M.DDocumento94 pagineCongestive Heart Failure CHF: Nik Nikam, M.DTia AriantiNessuna valutazione finora
- Cirrhosis 22008 Bajar Musica Gratis Descargar Musica Gratis Online Descargar Musica Gratis para CelularesDocumento72 pagineCirrhosis 22008 Bajar Musica Gratis Descargar Musica Gratis Online Descargar Musica Gratis para CelularesYeni Chie Aneuk TuleutNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Abraha AsfawDocumento303 pagineAbraha AsfawSaminas DemozNessuna valutazione finora
- Phil Iri Manual FinalDocumento422 paginePhil Iri Manual FinalMaam JoyceNessuna valutazione finora
- Curriculum and Pedagogy in Developing Country ContextsDocumento10 pagineCurriculum and Pedagogy in Developing Country ContextsTOBINessuna valutazione finora
- University of West Alabama 5E Lesson Plan Template: RL.6.4 SL.6.5 L.6.6)Documento2 pagineUniversity of West Alabama 5E Lesson Plan Template: RL.6.4 SL.6.5 L.6.6)api-423002246Nessuna valutazione finora
- Training & Certification UpdatesDocumento64 pagineTraining & Certification UpdatesRoger MachaNessuna valutazione finora
- Digital Society Guide enDocumento77 pagineDigital Society Guide enBelenNessuna valutazione finora
- Annotation Template For Teacher I-III (Proficient Teachers Objectives Means of Verification (MOV) Description of The MOV Presented AnnotationsDocumento5 pagineAnnotation Template For Teacher I-III (Proficient Teachers Objectives Means of Verification (MOV) Description of The MOV Presented AnnotationsJeffy P. UrbinaNessuna valutazione finora
- Microsoft Word - ICT - BookDocumento121 pagineMicrosoft Word - ICT - BookArthur MuseyaNessuna valutazione finora
- AITSL Application Guide Effective From 22 October 2013Documento8 pagineAITSL Application Guide Effective From 22 October 2013ahmedNessuna valutazione finora
- Mid Year IPCRF 2023 2024Documento12 pagineMid Year IPCRF 2023 2024A-jaye CelesenaNessuna valutazione finora
- Mil DLL July 10 - 14, 2017 Grade 12Documento4 pagineMil DLL July 10 - 14, 2017 Grade 12Jeoffrey Lance UsabalNessuna valutazione finora
- Assessment in Learning Ii: Rhea Micaila M. Generale CPE106 F14-2Documento32 pagineAssessment in Learning Ii: Rhea Micaila M. Generale CPE106 F14-2Rhea Micaila Maceda GeneraleNessuna valutazione finora
- Sara Carrico ResumeDocumento5 pagineSara Carrico ResumeSaraNessuna valutazione finora
- Curriculum Development For Medical EducationDocumento368 pagineCurriculum Development For Medical EducationMuhammed Elgasim93% (15)
- Assessment of Poor Learning Strategies and Their Effects On Academic Performance of Senior Secondary School Students in Sokoto StateDocumento6 pagineAssessment of Poor Learning Strategies and Their Effects On Academic Performance of Senior Secondary School Students in Sokoto StateIjahss JournalNessuna valutazione finora
- Chapter 4 Scaffolding Strategy RahmadiniDocumento45 pagineChapter 4 Scaffolding Strategy Rahmadinilaode rioNessuna valutazione finora
- Ell Lesson PlanDocumento3 pagineEll Lesson Planapi-270826504Nessuna valutazione finora
- Task 1 - Part B - Lesson Plans For Learning SegmentDocumento10 pagineTask 1 - Part B - Lesson Plans For Learning Segmentapi-217962443Nessuna valutazione finora
- Guide For Conducting Factory Capability Assessment For Power TransformersDocumento103 pagineGuide For Conducting Factory Capability Assessment For Power Transformersme_vahabi100% (2)
- Powerpoint Presentation RubricsDocumento26 paginePowerpoint Presentation RubricsISABEL GASESNessuna valutazione finora
- Syllabus For Assessment of Learning 1 (Prof Ed 606) (BEEd) PDFDocumento11 pagineSyllabus For Assessment of Learning 1 (Prof Ed 606) (BEEd) PDFMarbelyn Solomon LubosNessuna valutazione finora
- Frog Life Cycle Lesson PlanDocumento6 pagineFrog Life Cycle Lesson Planapi-300082815Nessuna valutazione finora
- My Practice Teaching PortfolioDocumento69 pagineMy Practice Teaching PortfolioDafchen Nio MahasolNessuna valutazione finora
- SW 3010Documento21 pagineSW 3010api-312630116Nessuna valutazione finora
- KL.9 ENGLISH HUB 3 First-Period-PlanningDocumento4 pagineKL.9 ENGLISH HUB 3 First-Period-PlanningAlbana Rama100% (2)
- ASL 1 Activity LeiiiiDocumento23 pagineASL 1 Activity LeiiiiEllaine DaprosaNessuna valutazione finora
- CG Carpentry For Grades 7-10Documento13 pagineCG Carpentry For Grades 7-10Em Israel Jr.100% (1)
- Carina Flores Calyeca SharingDocumento43 pagineCarina Flores Calyeca SharingDías Académicos Sharing SessionsNessuna valutazione finora
- Competencies and Professional Development Needs of Kindergarten TeachersDocumento13 pagineCompetencies and Professional Development Needs of Kindergarten TeachersManuel CaingcoyNessuna valutazione finora