Potrebbero piacerti anche
- Head InjuryDocumento2 pagineHead InjurySitta Grewo LiandarNessuna valutazione finora
- CBC Blood Chemistry ECG Chest X-Ray Extremity X-Ray UrinalysisDocumento2 pagineCBC Blood Chemistry ECG Chest X-Ray Extremity X-Ray UrinalysisSitta Grewo LiandarNessuna valutazione finora
- Pdu Agustus '15Documento125 paginePdu Agustus '15Sitta Grewo LiandarNessuna valutazione finora
- Assessment of Nutritional StatusDocumento3 pagineAssessment of Nutritional StatusSitta Grewo LiandarNessuna valutazione finora
- HYPERTENSIONDocumento55 pagineHYPERTENSIONCut Putri RiskaNessuna valutazione finora
- Nath PDFDocumento61 pagineNath PDFSitta Grewo LiandarNessuna valutazione finora
- Pdu Agustus '15Documento125 paginePdu Agustus '15Sitta Grewo LiandarNessuna valutazione finora
- Jogc PDFDocumento32 pagineJogc PDFnunki aprillitaNessuna valutazione finora
- Edinburgh Research Explorer: Cirrhosis: New Research Provides A Basis For Rational and Targeted TreatmentsDocumento6 pagineEdinburgh Research Explorer: Cirrhosis: New Research Provides A Basis For Rational and Targeted TreatmentsSitta Grewo LiandarNessuna valutazione finora
- WJG 20 7242Documento11 pagineWJG 20 7242Sitta Grewo LiandarNessuna valutazione finora
- 1632Documento5 pagine1632Sitta Grewo LiandarNessuna valutazione finora
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDocumento10 pagineSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionSitta Grewo LiandarNessuna valutazione finora
- HonkDocumento22 pagineHonkSitta Grewo LiandarNessuna valutazione finora
- WJG 20 7242Documento11 pagineWJG 20 7242Sitta Grewo LiandarNessuna valutazione finora
- Delivery of TwinsDocumento13 pagineDelivery of TwinsrhezzaagxxNessuna valutazione finora
- Ijms 15 10578Documento27 pagineIjms 15 10578Sitta Grewo LiandarNessuna valutazione finora
- Prevention of Maternal To Child Transmission of HivDocumento13 paginePrevention of Maternal To Child Transmission of HivSitta Grewo LiandarNessuna valutazione finora
- Caesarean SectionDocumento51 pagineCaesarean SectionFebrinata MahadikaNessuna valutazione finora
- Routine Infection Prevention: Infectio NDocumento62 pagineRoutine Infection Prevention: Infectio NSitta Grewo LiandarNessuna valutazione finora
- Hak-Hak Reproduksi WanitaDocumento38 pagineHak-Hak Reproduksi WanitafannyNessuna valutazione finora
- Routine Infection PreventionDocumento31 pagineRoutine Infection PreventionSitta Grewo LiandarNessuna valutazione finora
- Malaria in PregnancyDocumento18 pagineMalaria in PregnancySitta Grewo LiandarNessuna valutazione finora
- Routine Infection Prevention: Infectio NDocumento62 pagineRoutine Infection Prevention: Infectio NSitta Grewo LiandarNessuna valutazione finora
- Hak-Hak Reproduksi WanitaDocumento38 pagineHak-Hak Reproduksi WanitafannyNessuna valutazione finora
- Delivery of TwinsDocumento13 pagineDelivery of TwinsrhezzaagxxNessuna valutazione finora
- Delivery of TwinsDocumento13 pagineDelivery of TwinsrhezzaagxxNessuna valutazione finora
- Routine Infection PreventionDocumento31 pagineRoutine Infection PreventionSitta Grewo LiandarNessuna valutazione finora
- Why Do We Need ALARM CourseDocumento12 pagineWhy Do We Need ALARM CourseSitta Grewo LiandarNessuna valutazione finora
- Routine Infection Prevention: Infectio NDocumento62 pagineRoutine Infection Prevention: Infectio NSitta Grewo LiandarNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Salem RPGDocumento16 pagineSalem RPGabstockingNessuna valutazione finora
- Shell Gadus: Designed To Do More. Just Like Our Greases - Shell GadusDocumento2 pagineShell Gadus: Designed To Do More. Just Like Our Greases - Shell Gadusperi irawanNessuna valutazione finora
- Spectroscopy (L-26 To 29)Documento81 pagineSpectroscopy (L-26 To 29)Vashistha GargNessuna valutazione finora
- Nicholas Hudson - From Nation To Race: The Origin of Racial Classification in Eighteenth-CenturyDocumento19 pagineNicholas Hudson - From Nation To Race: The Origin of Racial Classification in Eighteenth-CenturyPedro IINessuna valutazione finora
- Zincanode 304 pc142Documento3 pagineZincanode 304 pc142kushar_geoNessuna valutazione finora
- Chemistry Notes: SUBJECT: Leaving Cert Chemistry Level: TEACHER: Tara LyonsDocumento5 pagineChemistry Notes: SUBJECT: Leaving Cert Chemistry Level: TEACHER: Tara LyonsSevinc NuriyevaNessuna valutazione finora
- Contact Inform 2002 PDFDocumento24 pagineContact Inform 2002 PDFFrank AlmeidaNessuna valutazione finora
- Sheet Metal Manufacturing Companies NoidaDocumento9 pagineSheet Metal Manufacturing Companies NoidaAmanda HoldenNessuna valutazione finora
- Bolt Action Italian Painting GuideDocumento7 pagineBolt Action Italian Painting GuideTirmcdhol100% (2)
- Modern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaDocumento2 pagineModern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaKumar KumarNessuna valutazione finora
- Aluminium Alloy - Wikipedia, The Free EncyclopediaDocumento12 pagineAluminium Alloy - Wikipedia, The Free EncyclopediaAshishJoshi100% (1)
- 04 SAMSS 005 Check ValvesDocumento9 pagine04 SAMSS 005 Check ValvesShino UlahannanNessuna valutazione finora
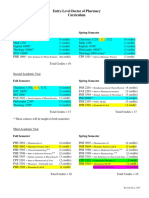
- Pharmd CurriculumDocumento18 paginePharmd Curriculum5377773Nessuna valutazione finora
- Fentanyl - Wikipedia, The Free EncyclopediaDocumento13 pagineFentanyl - Wikipedia, The Free EncyclopediaKeren SingamNessuna valutazione finora
- ODA X9 2SL DatasheetDocumento8 pagineODA X9 2SL DatasheetYudy UtamaNessuna valutazione finora
- JHS 182Documento137 pagineJHS 182harbhajan singhNessuna valutazione finora
- Procter and Gamble-1Documento5 pagineProcter and Gamble-1Abegiel MendozaNessuna valutazione finora
- Earth Sciences Notes Csir-Ugc Net JRFDocumento57 pagineEarth Sciences Notes Csir-Ugc Net JRFmanas773Nessuna valutazione finora
- Texto CuritibaDocumento1 paginaTexto CuritibaMargarida GuimaraesNessuna valutazione finora
- Zest O CorporationDocumento21 pagineZest O CorporationJhamane Chan53% (15)
- AR BuildingDocumento819 pagineAR BuildingShithin KrishnanNessuna valutazione finora
- By This Axe I Rule!Documento15 pagineBy This Axe I Rule!storm0% (1)
- Science Involved in Floating Paper Clip Science Experiment GuidelinesDocumento4 pagineScience Involved in Floating Paper Clip Science Experiment GuidelinesSHIELA RUBIONessuna valutazione finora
- 1986 EMT Disruption of Microbial Cells For Intracellular ProductsDocumento11 pagine1986 EMT Disruption of Microbial Cells For Intracellular ProductsLezid CortesNessuna valutazione finora
- TranscriptDocumento1 paginaTranscriptapi-310448954Nessuna valutazione finora
- Manufacuring EngineeringDocumento3 pagineManufacuring Engineeringapi-79207659Nessuna valutazione finora
- Updating - MTO I - Unit 2 ProblemsDocumento3 pagineUpdating - MTO I - Unit 2 ProblemsmaheshNessuna valutazione finora
- Relationsh Between EM and Young S ModuliDocumento7 pagineRelationsh Between EM and Young S ModuliDwight AndersonNessuna valutazione finora
- Tran-Effects of Assisted JumpingDocumento5 pagineTran-Effects of Assisted JumpingyoungjessNessuna valutazione finora
- Engineering Structures: C.X. Dong, A.K.H. Kwan, J.C.M. HoDocumento14 pagineEngineering Structures: C.X. Dong, A.K.H. Kwan, J.C.M. HoElieser SinagaNessuna valutazione finora