IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 6 Ver. III (Jun. 2015), PP 94-98
www.iosrjournals.org
High Sensitivity C-Reactive Protein In Patients With Acute
Injuries
Ayinbuomwan Ekiye,1 Idogun E.Sylvester,1 Iribhogbe Pius2
2.
1. Department Of Chemical Pathology University of Benin Teaching Hospital Benin-City, Nigeria
Department Of Trauma, Accident and Emergency, University of Benin Teaching Hospital Benin-City,
Nigeria
Correspondence: Ayinbuomwan Ekiye;
Abstract:
Background: C- reactive protein has been known as a highly sensitive but non-specific marker for acute
inflammation. The pattern of CRP response in trauma patients has not been evaluated in our environment.
Aim: The aim of the study was to determine the serial serum level of high sensitivity C- reactive protein (hsCRP) in patients with trauma.
Methods: This is a longitudinal study conducted at the University of Benin Teaching Hospital, Benin City,
Nigeria. One hundred and twenty patients with traumatic injuries were recruited at the accident and emergency
unit of UBTH and 30 apparently healthy individuals as controls. A structured questionnaire was administered to
all subjects to obtain demographics, injury type, tissue involvement and interventions. Samples were collected
from participants for estimation of h-sCRP on days 1, 3, and 8. hsCRP was analyzed using an ELISA method.
Results were analyzed with SPSS 16. P value was set at 0.05.
Results: A total of 116 patients and 30 controls completed the study. The most frequent cause of trauma
amongst the patients was vehicular crashes 80 (69.0%) followed by gunshot injuries 19 (16.4%). The mean
serum h-sCRP of the patients on the first day was (166.7 105.3mg/L) but it peaked on the third day post
trauma (373.4 131.2mg/L) and declined on the eighth day to 300.0 156.5mg/L) (P = <0.001).
Conclusion: C- reactive protein levels increase in the blood of trauma patients as a result of tissue damage but
decreased after the third day following trauma. However, in the presence of infection, the increase was
sustained. We therefore recommend that serial quantitative C-reactive protein measurements be done as an
adjunct to surgical care in patients with acute injuries.
Key Words: C-reactive protein, Trauma, Acute injuries, Benin City
I.
Introduction
C-reactive protein is an acute phase reactant synthesized in the liver. It was first described by Tillet and
Francis in 19301 as a substance present in the sera of acutely ill patients and able to bind the cell wall cpolysaccharide of Streptococcus pneumonia and agglutinate the organism. In 1941, the substance was shown to
be a protein and given the name C-reactive protein (CRP).1 Several studies have revealed that the risk of heartattack, stroke and other cardiovascular conditions is directly related to increasing levels of CRP. For many
years, CRP has been known as a highly sensitive but non-specific marker for acute inflammation and an
indicator of cardiovascular risk.1 CRP is known to rise to very high levels within 4-6 hours following acute
injurious conditions such as trauma, surgery, or infection. Increased serum CRP levels up to several-hundredfold are not uncommon after severe trauma. 2 Its level may rise in response to trauma such as burns, fractures or
surgery.3
CRP is known to increase in severe cases of inflammation and infection and drops as inflammation
subsides. It can therefore be useful in assessment of severity, metabolic response, prediction of outcome and
monitoring response in trauma patients.
Physical trauma is a leading cause of morbidity and mortality in all age groups, and post-traumatic
complications including infections which intensify inflammatory response abound. 4 Therefore, a parameter
helpful in monitoring inflammatory response and aiding early diagnosis of infections is not only advantageous
for early institution of treatment but also reduces morbidity and mortality to a large extent.
It has also been shown that daily quantitative analysis of CRP in blood of trauma patients allowed
prognosis of the development of nonbacterial systemic inflammation response, infectious complications and
sepsis.
CRP level >40mg/L on the first day (without use of glucocorticoids) suggest a risk of development of
infectious complications.5 Reduction of CRP from the third day is characteristic of a favorable course of
trauma.5 The onset of some infections may not be easily detected, especially if it is occult such as in the brain
and the bladder however rising or persistingly high CRP level may indicate complications. This study therefore
DOI: 10.9790/0853-14639498
www.iosrjournals.org
94 | Page
High Sensitivity C-Reactive Protein In Patients With Acute Injuries
aim to determine the serum levels of CRP in trauma patients on the first, third and eight day following trauma
and also assess serum CRP in the patients based on the nature of injury, tissue involvement and surgical
intervention.
II.
Methodology
Study Design: This is a longitudinal study conducted at the University of Benin Teaching Hospital,
Benin City, Nigeria.
Study Population: two groups of participants were recruited for this study including 120 patients with
traumatic injuries presenting to the accident and emergency unit of UBTH were recruited as the main study
population and 30 apparently healthy persons were recruited as controls.
A structured questionnaire was administered to all subjects to obtain demographic parameters, type of
injury, tissue involvement and intervention. Blood samples were collected from the patient group on days 1, 3
and 8 of presentation for evaluation of the pattern of CRP response in the study patients.
Inclusion Criteria: Subjects admitted within first 24hrs of injury; Age 16 65 years
Exclusion Criteria: Excluded from the study were patients with other medical conditions such as
diabetes mellitus, hypertension and any other condition that can generate inflammatory response.
Blood Sample Collection: Five milliliters of venous blood was collected from the antecubital veins and
dispensed into plain bottles for CRP estimation. The clotted blood was centrifuged at 2500 rpm for 10minutes
and the serum was separated into clean plain bottles and stored at -20C and analyzed within 2weeks of
collection.
hsCRP Assay: The high sensitivity C-reactive protein (hsCRP) ELISA is based on the principle of a
solid phase enzyme linked immunosorbent assay.6 The assay system utilizes a unique monoclonal antibody
directed against a distinct antigenic determinant on the CRP molecule.
Assay Characteristics: Assay was linear up to 10mg/L CRP. Acceptable coefficient of variation (CV)
was 20%. A standard of 10mg/L was analyzed in triplicates and the mean was found to be 10mg/L. The bias
was zero, giving an accuracy of 100%. A precision control of 50mg/L was analyzed ten times and the mean was
49.5%, standard deviation was 1.3 and coefficient of variation was 2.6%. Hence precision was 97.4%. Serum
samples demonstrating gross lipaemia, gross haemolysis or turbidity were not used with this test.
Data Analysis: Data were analyzed with statistical package for social science (SPSS) version 16.
Results were expressed as means, standard deviation and frequencies. The differences in means of CRP between
groups and subgroups were compared with students T- test and analysis of variation (ANOVA) as appropriate. P
value was set at 0.05.
III.
Results
A total of 150 subjects including 120 patient group and 30 controls were recruited. Four subjects in the
patient group died before day 8 sample was collected and were thus excluded. Thus 116 patients completed the
study. The mean age of trauma patients was 33.75 years and the controls 31.67 years (P > 0.05). Table 1 shows
the age groups and other demographics of the participants. Forty nine of the patients were withinn the age group
of 26 35 years representing the modal age group. Ninety four (81.0%) of the patients are males and 63
(54.3%) are singles.
Eighty (69.0%) of the patients had vehicular crashes, 19 (16.4%) had gunshot injuries, 8 (6.9%) had
burns injury, 4 (3.4%) each had assault and stab injuries. Fifty nine patients had soft tissue injuries while 57
sustained fracture. Fifteen (12.9%) of the them had surgical intervention among other treatment modalities.
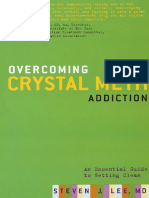
Table 2 and fig. 1 shows the mean and standard deviation of the hsCRP values on days 1, 3 and 8 post
injury and those of the controls. hsCRP levels is significantly higher in patient group compared to controls. The
value increased significantly by day 3 (peak) and decreased by day 8 though day the 8 value was still higher
than day 1. This was the trend in all the injury subtypes except in the patients with burns and assault related
injuries as shown in table 3 in whom CRP level continued to increase even on day 8. The changes in the
subgroup with assault injuries did not show any significant difference in mean CRP despite the increament.
Comparing CRP levels on each of the days evaluated between the injury subtypes, the mean levels of
CRP on days 1 and 3 did not differ significantly between the subgroups but the mean CRP of the patients with
stab injuries dropped significantly on day 8 compared to the others as shown in table 4
Based on tissue involvement, CRP levels increased on day 1, peaks at day 3 and declines by day 8 in
subjects with soft tissue and bone involvements as shown in table 5. There is no significant difference in the
mean level of CRP on each day between those with soft tissue and bone injuries as shown in table 6.
Similarly, the mean CRP significantly increased by day 3 and 8 however the day 8 CRP was lower than
day 3 in patients who had surgery as well as those who did not as shown in table 5. CRP levels were
significantly higher in the subgroup without surgical intervention on day 1 but the group that had surgery had a
significantly higher day 3 CRP as shown on table 6.
DOI: 10.9790/0853-14639498
www.iosrjournals.org
95 | Page
High Sensitivity C-Reactive Protein In Patients With Acute Injuries
IV.
Discussion
CRP levels rise in serum or plasma within 24-48hrs following acute tissue damage, peaks during the
acute stage and decrease with the resolution of inflammation or trauma.7 In the index study, we found that CRP
levels were significantly higher than controls within 24 hrs of injury, peaked by day 3 and declined by day 8 in
all types of physical injuries except in patients with burns and assault related injuries in whom CRP remained
persistently high even at day 8.
This marked rise in CRP levels from day 1-3 followed by its decline on day 8, is in keeping with
previous studies by Claudia et al8 and Gupta et al3. The maximal generation of CRP on the third day can be
linked to high levels of circulating IL-6 release which evidently precedes the equivalent production of CRP by at
least 12 hours.9 This maximal generation of CRP has been described by Ertel et al.10
CRP level is known to reflect the impact of trauma on the body and associated tissue damage. 11 The
time course of trauma induced CRP production in general goes along with a gap of several hours. As a
consequence, elevated CRP levels were more pronounced on the third day irrespective of the degree of tissue
damage. However the exception observed in patients who had burns may suggest the presence of infection as a
complication. Burns is associated with a high risk of infection due to extensive breakdown of the barrier defence
mechanism of the body. Studies by Jeschke et al12 showed that CRP levels may continue to increase beyond day
8 before it declines though they concluded that CRP may not predict sepsis in burns patients. This observation
was corroborated by Pileri et al13 who showed that CRP increases till day 15 before declining.
When patients with fractures were compared with those who had soft tissue injuries, there was no
significant difference in the mean CRP levels in the two groups. This may suggest that CRP response is not
dependent on the tissue type involved rather it is the degree of tissue damage that may determine the
inflammatory response and therefore CRP levels. 9
Results from this study showed that CRP levels were higher for patients who had surgery than for those
who did not on day 3. It has been reported that CRP rises early after surgical intervention.14 The rise in CRP
after surgical intervention is expected because of tissue injury and associated inflammatory response however
persistently elevated CRP may become a biological warning sign, which should raise an index of suspicion for
infection.3
V.
Conclusion
In conclusion, CRP level increases in the blood of trauma patients as a result of tissue damage but
decreases after the third day following trauma. However, a sustained increase should be properly investigated as
it may suggest complication by infection. We therefore recommend that serial quantitative CRP measurements
be done as an adjunct to surgical care in patients with acute injuries.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
[14].
Nadar Rifai and Russel Warnick: Lipids, lipoproteins, apolipoproteins, and other cardiovascular risk factors. In Tietz Textbook of
Clinical chemistry and molecular diagnosis. 4 th ed. Carl Burtis, Edward Ashwood, David Bruns. Elsevier Inc. New Delhi. 2006; 962
963.
Pritchett JW. Creactive protein levels determine the severity of soft tissue injuries. Am J. Orthop. 1996 ; 25: 759-761.
Gupta R, Singh S, Soni M. C- reactive protein as an indicator of sepsis in orthopedic trauma. India J Med Sci. 2002; 56: 501-507.
El Hassan BS, Peak JD, Wicher JT, Shepherd J. Acute phase protein levels as an index of severity of physical injury. Int J Oral
Maxillofac. Surg. 1990; 19: 346 349.
Gumanenko EK, Nemchenko NS, Boyarin. Tsev VV, Nikiforenko AV, Pavlenko AN, Rud AA. C- reactive protein in severe trauma
not complicated and complicated by sepsis. Vestnik Hirurgii im. I.I Grekova. 2005; 164(5): 55-59.
Whicher JT. BCR/IRMM reference material for plasma (CRM 470). Clin Biochem 1998; 31: 459-465.
Shine B. de Beer F.C, Pepys M.B. Solid phase radioimmunoassay for human C-reactive protein. J Lab Clinica Chimica Acta 1981;
117: 13 23.
Claudia M, Lili K, Thomas S, Stefan W, Christian J, Oswald F, et al. C-reactive Protein and All Cause Mortality in a Large
Hospital - based Cohort. Clin Chem 2008; 54: 343-349.
Florian G, Helga P, Gerald S, Wolf S, Lother K, Uwe BB. Is Interleukin 6 an Early Marker of Injury Severity following major
Trauma in Humans? Arch Surg. 2000; 135: 291-295.
Ertel W, Faist E, Nestle C. Kinetics of Interleukin - 2 and Interleukin - 6 synthesis following major mechanical trauma. J Surg Res.
1990; 48: 622-628.
Bewster N, Guthrie C, McBirnie J. CRP levels as a measure of surgical trauma: a comparison of different general surgical
procedures. J R Coll Surg Edinb 1994; 39: 86-88.
Jeschke MG, Finnerty CC, Kulp GA, Kraft R, Herndon DN. Can we use CRP levels to predict severe infection or sepsis in severely
burned patients? Int J Burns Trauma. 2013; 3(3): 137-143.
Pileri D, Accardo-Palumbo A, DAmelio L, DArpa N et al. Serum levels of cortisol, Immunoglobulin and CRP in burn patients. Ann
Burns Fire Disasters. 2009; 22 (1): 3 5.
Neumaier M, Metak G, Scherer M.A. C-reactive protein as a parameter of surgical trauma: CRP response after different types of
surgery in 349 hip fractures. Acta Orthopaedica 2006; 77(5): 788-790.
DOI: 10.9790/0853-14639498
www.iosrjournals.org
96 | Page
High Sensitivity C-Reactive Protein In Patients With Acute Injuries
2. List of Tables
Table 1: Demographic Parameters of the Study Populace
Variables
Age group
16 25
26 35
36 45
46 55
56 65
Patient Group
Control Group
31 (26.7)
49 (42.2)
20 (17.2)
6 (5.2)
10 (8.6)
7 (23.3)
15 (50.0)
7 (23.3)
1 (3.3)
0 (0.0)
94 (81.0)
22 (19.0)
19 (63.3)
11 (36.7)
63 (54.3)
53 (45.7)
15 (50.0)
15 (50.0)
Sex
Male
Female
Marital Status
Single
Married
Level of Education
None
Primary
Secondary
Tertiary
23 (19.8)
27 (23.3)
38 (32.8)
28 (24.1)
Table 2: Mean SD of CRP in Patients and Controls
Variables
Patient Group
Day 1
CRP
Control
Day 3
P value
Day 8
Mean SD
Mean SD
Mean SD
Mean SD
166.7 105.3**
373.4 131.2**
300.0 156.5**
69.4 68.1
<0.001
Table 3: Changes in CRP based on Injury Subtype
Variables
Type of Injury
RTA
Gunshot
Burns
Assault
Stab
Grinder
Freq.(%)
n=116
80 (69.0)
19 (16.4)
8 (6.9)
4 (3.4)
4 (3.4)
1 (0.9)
Day 1
Mean SD
181.6 105.7
130.4 104.8
108.5 84.2
196.7 135.6
140.7 64.1
118.3
Day 3
Mean SD
365.1 132.9
422.7 102.1
362.9 187.9
254.6 74.7
416.5 13.0
497.8
Day 8
Mean SD
281.3 154.0
361.9 157.7
424.0 84.6
323.9 150.2
108.5 40.1
295.1
P value
0.001
0.001
0.001
0.391
0.001
NA
Table 4: Comparism of the difference in mean CRP in the subgroups on each study day
Days
Assault
RTA
Gunshot
Burns
Stab
P value
196.7 135.6
181.6 105.7
130.4 104.8
108.5 84.2
140.7 64.1
0.144
254.6 74.7
365.1 132.9
422.7 102.1
362.9 187.9
416.5 13.0
0.148
323.9 150.2
281.3 154.0
361.9 157.7
424.0 84.6
108.5 40.1
**
0.003
Table 5: Changes in mean CRP based on tissue involvement and surgical intervention with time
Table 6: Comparism of changes in CRP on each day based on Tissue Involvement and Surgical
Intervention
DOI: 10.9790/0853-14639498
www.iosrjournals.org
97 | Page
High Sensitivity C-Reactive Protein In Patients With Acute Injuries
List of Figures
Figure 1: Changes in mean hsCRP levels with time in each subgroup.
DOI: 10.9790/0853-14639498
www.iosrjournals.org
98 | Page
Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- Overcoming Crystal Meth Addiction An Essential Guide To Getting Clean From CM AddictionDocumento444 pagineOvercoming Crystal Meth Addiction An Essential Guide To Getting Clean From CM Addictionrey_colón_5100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationDocumento6 pagineKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Acute Kidney Injury W/ Hyperkalemia NCPDocumento5 pagineAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenNessuna valutazione finora
- Dental Public HealthDocumento264 pagineDental Public HealthCorina Manole DanielaNessuna valutazione finora
- Human Rights and Dalits: Different Strands in The DiscourseDocumento5 pagineHuman Rights and Dalits: Different Strands in The DiscourseInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Full-Mouth Adhesive Rehabilitation in Case of Severe Dental Erosion, A Minimally Invasive Approach Following The 3-Step TechniqueDocumento18 pagineFull-Mouth Adhesive Rehabilitation in Case of Severe Dental Erosion, A Minimally Invasive Approach Following The 3-Step TechniqueHoracio Mendia100% (1)
- Blood Bank ChecklistDocumento4 pagineBlood Bank ChecklistFIAZ MAQBOOL FAZILINessuna valutazione finora
- The Impact of Technologies On Society: A ReviewDocumento5 pagineThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- 861 Drug Prescribing For Dentistry 2 Web 2 Email PDFDocumento94 pagine861 Drug Prescribing For Dentistry 2 Web 2 Email PDFRaphaela TravassosNessuna valutazione finora
- Nephrons (Functional Unit)Documento44 pagineNephrons (Functional Unit)Nur SanaaniNessuna valutazione finora
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDocumento7 pagineSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDocumento6 pagineThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDocumento5 pagine"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDocumento7 pagineA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDocumento5 pagineAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Documento15 pagineA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDocumento4 pagineInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- The Lute Against Doping in SportDocumento5 pagineThe Lute Against Doping in SportInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDocumento14 pagineAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Assessment of The Implementation of Federal Character in Nigeria.Documento5 pagineAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDocumento7 pagineTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDocumento5 pagineEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDocumento7 pagineComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDocumento5 pagineRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Transforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweDocumento9 pagineTransforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Importance of Mass Media in Communicating Health Messages: An AnalysisDocumento6 pagineImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDocumento5 pagineDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalNessuna valutazione finora
- Beowulf: A Folktale and History of Anglo-Saxon Life and CivilizationDocumento3 pagineBeowulf: A Folktale and History of Anglo-Saxon Life and CivilizationInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Role of Madarsa Education in Empowerment of Muslims in IndiaDocumento6 pagineRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Micro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaDocumento3 pagineMicro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- An Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsDocumento6 pagineAn Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Classical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahDocumento9 pagineClassical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Women Empowerment Through Open and Distance Learning in ZimbabweDocumento8 pagineWomen Empowerment Through Open and Distance Learning in ZimbabweInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Substance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaDocumento11 pagineSubstance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Motivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweDocumento8 pagineMotivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- A Study On The Television Programmes Popularity Among Chennai Urban WomenDocumento7 pagineA Study On The Television Programmes Popularity Among Chennai Urban WomenInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Design Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextDocumento6 pagineDesign Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Monthly Accomplishment FormDocumento2 pagineMonthly Accomplishment FormflyaxizsNessuna valutazione finora
- Community Health and Program Services (CHAPS) : Health Disparities Among Racial/Ethnic PopulationsDocumento4 pagineCommunity Health and Program Services (CHAPS) : Health Disparities Among Racial/Ethnic PopulationsMuhammad Bachiar SafrudinNessuna valutazione finora
- Acute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsDocumento2 pagineAcute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsSachin SinghNessuna valutazione finora
- UAS Genap Semester II Kebidanan STIKES HafshawatyDocumento3 pagineUAS Genap Semester II Kebidanan STIKES HafshawatyHanna HannaNessuna valutazione finora
- Htmle Diagnostic Exam RatioDocumento18 pagineHtmle Diagnostic Exam RatioAlliah Jessa PascuaNessuna valutazione finora
- 42fundus AngiographyDocumento28 pagine42fundus AngiographyHitesh SharmaNessuna valutazione finora
- FOAT Readings and ResourcesDocumento1 paginaFOAT Readings and Resourcesagnes windramNessuna valutazione finora
- Introduction To Nursing PharmacologyDocumento5 pagineIntroduction To Nursing PharmacologyJon Adam Bermudez SamatraNessuna valutazione finora
- Past PapaersDocumento515 paginePast PapaersShariq ShaNessuna valutazione finora
- Delafloxacin 4Documento23 pagineDelafloxacin 4Muhammad RamzanNessuna valutazione finora
- Cervical Lymphoepithelial CystDocumento6 pagineCervical Lymphoepithelial CystAhmed Al-jumailiNessuna valutazione finora
- TimeWise Miracle Set 3D Fact Sheet MYSG ENGDocumento2 pagineTimeWise Miracle Set 3D Fact Sheet MYSG ENGKilinSilinNessuna valutazione finora
- History of HIVDocumento4 pagineHistory of HIVHyrum KamandeNessuna valutazione finora
- Nursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDocumento5 pagineNursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDr-Marudhar MarudharNessuna valutazione finora
- Mgi Presentation - ReyDocumento65 pagineMgi Presentation - ReyCharlot Jade Paderes67% (3)
- Choose 2 From The Disease Below That Are Emerging in The PhilippinesDocumento4 pagineChoose 2 From The Disease Below That Are Emerging in The PhilippinesMICHELLE BIANCA PATRICE CRUZNessuna valutazione finora
- HematologyDocumento100 pagineHematologyerzaraptorNessuna valutazione finora
- DUODENAL PROCEDUREDocumento5 pagineDUODENAL PROCEDUREeka nurjanahNessuna valutazione finora
- Femur and Pelvis Fracture (Trauma)Documento20 pagineFemur and Pelvis Fracture (Trauma)Ree YahNessuna valutazione finora
- Dental CatalogueDocumento28 pagineDental CataloguePaulus LagadanNessuna valutazione finora
- Introducing The Epidermis.: ReallyDocumento47 pagineIntroducing The Epidermis.: ReallyNaila JinNessuna valutazione finora
- Blood and Tissue Coccidian GuideDocumento40 pagineBlood and Tissue Coccidian GuideMichael DawitNessuna valutazione finora
- 2017 Ayurvedic Concept of ShatkriyakalaDocumento8 pagine2017 Ayurvedic Concept of ShatkriyakalaTúlio Laraia CoutinhoNessuna valutazione finora