Potrebbero piacerti anche
- Heavy HandsDocumento8 pagineHeavy HandsPicklehead McSpazatronNessuna valutazione finora
- Petroleum Industry Act 2021 Key Highlights 230821Documento33 paginePetroleum Industry Act 2021 Key Highlights 230821Ebene ChimaNessuna valutazione finora
- Petroleum DPRDocumento45 paginePetroleum DPROgbu ObioraNessuna valutazione finora
- Mind Control Forums - Complete Book ListDocumento11 pagineMind Control Forums - Complete Book ListSimon Benjamin100% (2)
- Clinical Massage Therapy - S. Jurch Hill, 2009) WWDocumento562 pagineClinical Massage Therapy - S. Jurch Hill, 2009) WWMohsen Bt92% (12)
- Construction and Projects in Qatar OverviewDocumento27 pagineConstruction and Projects in Qatar Overviewfaleela IsmailNessuna valutazione finora
- Uae Oil & GasDocumento18 pagineUae Oil & GasAna MarksNessuna valutazione finora
- National Iranian Oil CompanyDocumento8 pagineNational Iranian Oil CompanyMatheus RochaNessuna valutazione finora
- Petrochemicals and The Vision 2030Documento13 paginePetrochemicals and The Vision 2030vasucristalNessuna valutazione finora
- PetroChina 2010 Annual ReportDocumento236 paginePetroChina 2010 Annual ReportNeal Shah100% (1)
- Energy Briefs - Middle East Refinery AdditionsDocumento5 pagineEnergy Briefs - Middle East Refinery AdditionsNikhil JainNessuna valutazione finora
- War Dogs 1Documento26 pagineWar Dogs 1api-340421195Nessuna valutazione finora
- ALCAD Ni-CD BatteriesDocumento8 pagineALCAD Ni-CD BatteriesVikrantNessuna valutazione finora
- Dmart in UAEDocumento19 pagineDmart in UAEPriti SawantNessuna valutazione finora
- Dokumen - Tips Fuel Oil Loading System Upgrade at Yanbu Refinery June 2016 Enppifuel OilDocumento24 pagineDokumen - Tips Fuel Oil Loading System Upgrade at Yanbu Refinery June 2016 Enppifuel Oilafs araeNessuna valutazione finora
- Safety of Oil Installations Standing Committee ReportDocumento96 pagineSafety of Oil Installations Standing Committee ReportVaishnavi Jayakumar100% (1)
- Oil and Gas Company ProfileDocumento3 pagineOil and Gas Company Profileayush gandhiNessuna valutazione finora
- Module 5 Cognitive Mental AssessmentDocumento12 pagineModule 5 Cognitive Mental Assessmentlagathurc100% (2)
- Pneumatic Oil Security Data SheetDocumento4 paginePneumatic Oil Security Data SheetSayed Diab AlsayedNessuna valutazione finora
- Pipeline2007 PDFDocumento0 paginePipeline2007 PDFsinyoprimaNessuna valutazione finora
- (RRL - 1) Spent Bleaching Earth Extraction FAQSDocumento4 pagine(RRL - 1) Spent Bleaching Earth Extraction FAQSShania LoveresNessuna valutazione finora
- BYCO ReportDocumento17 pagineBYCO ReportAliRashidNessuna valutazione finora
- Child Psychiatric EmergenciesDocumento8 pagineChild Psychiatric EmergenciesDanitza YhovannaNessuna valutazione finora
- International Symposium On Safety Instrumentation in Oil & Gas IndustryDocumento4 pagineInternational Symposium On Safety Instrumentation in Oil & Gas Industrysong LiNessuna valutazione finora
- Orica Kurri ANE Appendix-10 GreenhouseDocumento45 pagineOrica Kurri ANE Appendix-10 GreenhouselladopiNessuna valutazione finora
- 2021 Sustainability FinalDocumento36 pagine2021 Sustainability FinalLovely ChoudharyNessuna valutazione finora
- Japanese EncephalitisDocumento9 pagineJapanese EncephalitisAhmed Mawardi0% (1)
- 1200h Medw Samir PresentationDocumento26 pagine1200h Medw Samir PresentationRobert LopezNessuna valutazione finora
- The Nigerian Gas Master Plan As Presented by NNPC in 2008Documento39 pagineThe Nigerian Gas Master Plan As Presented by NNPC in 2008Adedire FisayoNessuna valutazione finora
- Introdiction To Engineering PDFDocumento295 pagineIntrodiction To Engineering PDFAyebareNessuna valutazione finora
- Engineering Dreams: A Career in Any Stream of Engineering Is Equally Fruitful and RewardingDocumento4 pagineEngineering Dreams: A Career in Any Stream of Engineering Is Equally Fruitful and RewardingRamPrasadMeenaNessuna valutazione finora
- OGDCL Trainee Test 2017Documento3 pagineOGDCL Trainee Test 2017Ali AhmadNessuna valutazione finora
- MSDS - GulfSea Compressor Oils PDFDocumento5 pagineMSDS - GulfSea Compressor Oils PDFObydur RahmanNessuna valutazione finora
- Used OilDocumento11 pagineUsed Oilrvsingh100% (3)
- Azeem CVDocumento2 pagineAzeem CVAtiq Ur RehmanNessuna valutazione finora
- Curriculam Vitae: Mohammed - Alfaz AliDocumento6 pagineCurriculam Vitae: Mohammed - Alfaz Alirj4ronyNessuna valutazione finora
- Oil and Gas Company Profile PDFDocumento2 pagineOil and Gas Company Profile PDFChandrashekharCSKNessuna valutazione finora
- RICI Brochure CompressedDocumento27 pagineRICI Brochure CompressedFaris AhmedNessuna valutazione finora
- OGP Safety Performance Indicators 2005Documento116 pagineOGP Safety Performance Indicators 2005kave4923Nessuna valutazione finora
- Syaukani Muhammad AliDocumento6 pagineSyaukani Muhammad AlidotcomNessuna valutazione finora
- MSDS PetrolDocumento6 pagineMSDS PetrolridgellNessuna valutazione finora
- Sample Project ProposalDocumento26 pagineSample Project ProposalNithinKallayilNessuna valutazione finora
- Radicalization and The Use of Social MediaDocumento26 pagineRadicalization and The Use of Social MediaSaad BalochNessuna valutazione finora
- Seminar ReportDocumento21 pagineSeminar ReportEr Gaurav Agrawal100% (3)
- Top 100 Oil and Gas Operators PDFDocumento6 pagineTop 100 Oil and Gas Operators PDFNur Syaffiqa Mohamad RuzlanNessuna valutazione finora
- MSDS - GulfSea Gear Oil@Documento4 pagineMSDS - GulfSea Gear Oil@Obydur RahmanNessuna valutazione finora
- OngcDocumento518 pagineOngcUday KumarNessuna valutazione finora
- CV of Eng. ShehabDocumento4 pagineCV of Eng. ShehabAhmed SlamNessuna valutazione finora
- DARFAPDocumento13 pagineDARFAPSamanthaLWildtNessuna valutazione finora
- CSR & Sustainable Development PresentationDocumento13 pagineCSR & Sustainable Development PresentationArnav BothraNessuna valutazione finora
- Chemical Industry in Turkey by Selcuk DenizhanDocumento10 pagineChemical Industry in Turkey by Selcuk DenizhanSelcuk DenizhanNessuna valutazione finora
- Writing Test 1-4Documento8 pagineWriting Test 1-4KashaypNessuna valutazione finora
- Oman Health System ProfileDocumento58 pagineOman Health System ProfileToufiq_duNessuna valutazione finora
- Essentials of Houe and 5sDocumento2 pagineEssentials of Houe and 5sRajesh Kumar SinghNessuna valutazione finora
- If You Are Not Connected To The VINCI Energies Network (Outside The Business Unit's Premises)Documento16 pagineIf You Are Not Connected To The VINCI Energies Network (Outside The Business Unit's Premises)Fendi ahmadNessuna valutazione finora
- Oil Industry in Japan (Ken-Morota)Documento67 pagineOil Industry in Japan (Ken-Morota)Hoang ThangNessuna valutazione finora
- 13 Very Important Type Tests of A Low Voltage Switchgear Carried Out by The ManufacturerDocumento10 pagine13 Very Important Type Tests of A Low Voltage Switchgear Carried Out by The ManufacturerAhmed BoussoffaraNessuna valutazione finora
- Clean Fuels Manual PDFDocumento182 pagineClean Fuels Manual PDFbennimitz100% (1)
- Job SearchDocumento7 pagineJob SearchPartheeban SkpNessuna valutazione finora
- Nestle Annual Report Management 2020Documento128 pagineNestle Annual Report Management 2020Aziz ur RehmanNessuna valutazione finora
- SNGPL TestDocumento4 pagineSNGPL Testsajjad aliNessuna valutazione finora
- Amish Iocl Barauni MainDocumento16 pagineAmish Iocl Barauni Mainamish umar0% (1)
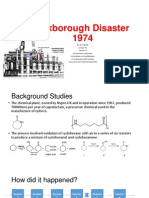
- Flixborough Disaster PresentationDocumento6 pagineFlixborough Disaster PresentationTan Yong ChaiNessuna valutazione finora
- Seborrheic Dermatitis From JurnalDocumento6 pagineSeborrheic Dermatitis From JurnalindciwNessuna valutazione finora
- Dermatitis SeborreicaDocumento6 pagineDermatitis SeborreicaDiego Eraso IncaNessuna valutazione finora
- Seborrheic Dermatitis in Adolescents and AdultsDocumento51 pagineSeborrheic Dermatitis in Adolescents and AdultsCosmina GeorgianaNessuna valutazione finora
- Dermatitis Seborroeik: DR Maria Dwikarya SPKKDocumento22 pagineDermatitis Seborroeik: DR Maria Dwikarya SPKKHendy MasjayantoNessuna valutazione finora
- Embedded and Impacted TeethDocumento2 pagineEmbedded and Impacted TeethAhmed MawardiNessuna valutazione finora
- 5f97a6778781eDocumento1 pagina5f97a6778781eAhmed MawardiNessuna valutazione finora
- 5f97a6778781eDocumento1 pagina5f97a6778781eAhmed MawardiNessuna valutazione finora
- Pedoman DMDocumento32 paginePedoman DMPon_Zi_cuteNessuna valutazione finora
- Pedoman DMDocumento32 paginePedoman DMPon_Zi_cuteNessuna valutazione finora
- Ahmed MawardiDocumento1 paginaAhmed MawardiAhmed MawardiNessuna valutazione finora
- Ahmed Mawardi: ObjectiveDocumento1 paginaAhmed Mawardi: ObjectiveAhmed MawardiNessuna valutazione finora
- ADocumento5 pagineAAhmed MawardiNessuna valutazione finora
- A Comparison of Hair Quality and Cosmetic AcceptanceDocumento4 pagineA Comparison of Hair Quality and Cosmetic AcceptanceAhmed MawardiNessuna valutazione finora
- Toefl Answer Sheet For Free Test: NoteDocumento4 pagineToefl Answer Sheet For Free Test: NoteAhmed MawardiNessuna valutazione finora
- Treatment of Seborrheic Dermatitis PDFDocumento7 pagineTreatment of Seborrheic Dermatitis PDFAhmed MawardiNessuna valutazione finora
- CHT Hfa Boys P 2 5Documento1 paginaCHT Hfa Boys P 2 5Dillon WilsonNessuna valutazione finora
- Billing Statement 1Documento3 pagineBilling Statement 1Ahmed MawardiNessuna valutazione finora
- Presentation 1Documento2 paginePresentation 1Ahmed MawardiNessuna valutazione finora
- A Practical Guide To Scalp DisorderDocumento5 pagineA Practical Guide To Scalp DisorderAhmed MawardiNessuna valutazione finora
- 21 PDFDocumento39 pagine21 PDFAhmed MawardiNessuna valutazione finora
- 2086 Genome FinalDocumento1 pagina2086 Genome FinalAhmed MawardiNessuna valutazione finora
- ADocumento5 pagineAAhmed MawardiNessuna valutazione finora
- 21 PDFDocumento39 pagine21 PDFAhmed MawardiNessuna valutazione finora
- Emd166 Slide Shock-1Documento53 pagineEmd166 Slide Shock-1THuthi MUktiNessuna valutazione finora
- Three Etiologic Facets of Dandruff and Seborrheic Dermatitis: Malassezia Fungi, Sebaceous Lipids, and Individual SensitivityDocumento3 pagineThree Etiologic Facets of Dandruff and Seborrheic Dermatitis: Malassezia Fungi, Sebaceous Lipids, and Individual SensitivityAhmed MawardiNessuna valutazione finora
- ADocumento4 pagineAAhmed MawardiNessuna valutazione finora
- Dandruff Has An Altered Stratum CorneumDocumento7 pagineDandruff Has An Altered Stratum CorneumAhmed MawardiNessuna valutazione finora
- Presentation 1Documento4 paginePresentation 1Ahmed MawardiNessuna valutazione finora
- Cancer Epidemiology: Hematology Oncology Division Child Health Departement - Universty of Sumatera UtaraDocumento27 pagineCancer Epidemiology: Hematology Oncology Division Child Health Departement - Universty of Sumatera Utaraparik2321Nessuna valutazione finora
- Katz and Fischer - The Revised International Health RegulationsDocumento18 pagineKatz and Fischer - The Revised International Health RegulationsAhmed MawardiNessuna valutazione finora
- Scaling Up Nutrition A Framework For ActionDocumento1 paginaScaling Up Nutrition A Framework For ActionAhmed MawardiNessuna valutazione finora
- FM k36 Prenatal CareDocumento33 pagineFM k36 Prenatal CareAhmed MawardiNessuna valutazione finora
- Acr Bi-Rads Atlas 5 Edition ChangesDocumento7 pagineAcr Bi-Rads Atlas 5 Edition ChangesDiego SánchezNessuna valutazione finora
- Submitted By: TOOBA SAEED - 70074236: Natural Holistic Healing and Wellness CenterDocumento4 pagineSubmitted By: TOOBA SAEED - 70074236: Natural Holistic Healing and Wellness CenterTooba SaeedNessuna valutazione finora
- 18c. Lymphoma EditedDocumento36 pagine18c. Lymphoma EditedMUHAMMAD BAGIR ALJUFRINessuna valutazione finora
- Program and Proceedings - 23rd International "STRESS AND BEHAVIOR" Neuroscience and Biopsychiatry Conference, St-Petersburg, Russia (May 16-19, 2016)Documento56 pagineProgram and Proceedings - 23rd International "STRESS AND BEHAVIOR" Neuroscience and Biopsychiatry Conference, St-Petersburg, Russia (May 16-19, 2016)ISBS_SocietyNessuna valutazione finora
- Master Kinesiotaping HandoutDocumento11 pagineMaster Kinesiotaping HandoutcosasdeangelNessuna valutazione finora
- Hemo PathDocumento2 pagineHemo PathanadiguptaNessuna valutazione finora
- Strabismus and Diplopia After Refractive SurgeryDocumento5 pagineStrabismus and Diplopia After Refractive Surgeryyuda saputraNessuna valutazione finora
- Nursing Process of A Client With CholelithiasisDocumento21 pagineNursing Process of A Client With Cholelithiasisapi-3822508100% (6)
- Bns 209 Module 6 Prevention in Hiv and AidsDocumento12 pagineBns 209 Module 6 Prevention in Hiv and AidslebogangNessuna valutazione finora
- Catalogue v09Documento4 pagineCatalogue v09KRISHNA L BAISETTINessuna valutazione finora
- Addiction and GroupDocumento2 pagineAddiction and GrouproxanarNessuna valutazione finora
- M1 Introduction To Manual TherapyDocumento101 pagineM1 Introduction To Manual TherapySylvia LoongNessuna valutazione finora
- Preliminary Study Evaluating Tests Used To Diagnose Canine Cranial Cruciate Ligament FailureDocumento4 paginePreliminary Study Evaluating Tests Used To Diagnose Canine Cranial Cruciate Ligament FailureCesar AlvearNessuna valutazione finora
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Documento4 pagineComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangNessuna valutazione finora
- Pediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467LDocumento4 paginePediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467Lapi-324566318Nessuna valutazione finora
- HIS Primary HospitalDocumento7 pagineHIS Primary HospitalJaaaaaaaaazNessuna valutazione finora
- Steam Distilation PDFDocumento9 pagineSteam Distilation PDFAlam LazuardiNessuna valutazione finora
- ADN Care Plan - DepressionDocumento3 pagineADN Care Plan - DepressionDavid PerezNessuna valutazione finora
- Glimpse of My ResearchDocumento4 pagineGlimpse of My Researchमनोज जैनNessuna valutazione finora
- Sleep Apnea Research PaperDocumento9 pagineSleep Apnea Research Paperaflbuagdw100% (3)
- What Is A CT ScanDocumento3 pagineWhat Is A CT ScanZackNessuna valutazione finora
- European Waste Catalogue AND Hazardous Waste List: Valid From 1 January 2002Documento49 pagineEuropean Waste Catalogue AND Hazardous Waste List: Valid From 1 January 2002Mark VellaNessuna valutazione finora
- Patient and Family Guide To The CANMAT and ISBD Guidelines On The Management of Bipolar DisorderDocumento34 paginePatient and Family Guide To The CANMAT and ISBD Guidelines On The Management of Bipolar DisorderLucila VialeNessuna valutazione finora
- Finalpaper SchnakeDocumento6 pagineFinalpaper Schnakeapi-315989347Nessuna valutazione finora