Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Newborn Antibiotic Guide or Early and Late Onset Sepsis During Birth Episode of Care Revised June 2018Documento14 pagineNewborn Antibiotic Guide or Early and Late Onset Sepsis During Birth Episode of Care Revised June 2018Raiyan KhanNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Denosumab in MyelomaDocumento5 pagineDenosumab in MyelomaRaiyan KhanNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Miracle Baby: Managing Extremely Preterm Birth in Rural UgandaDocumento4 pagineMiracle Baby: Managing Extremely Preterm Birth in Rural UgandaRaiyan KhanNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Sample Strong Eras Lor 5-05Documento1 paginaSample Strong Eras Lor 5-05Raiyan KhanNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Prepare For Blood Donation Flyer A4Documento1 paginaPrepare For Blood Donation Flyer A4Raiyan KhanNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Health Pra CRN at LawDocumento313 pagineHealth Pra CRN at LawRaiyan KhanNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Notification Form NOTF 00Documento10 pagineNotification Form NOTF 00Raiyan KhanNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- LicenseDocumento3 pagineLicenseSourav SharmaNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
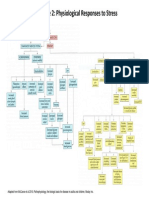
- Figure 2: Physiological Responses To StressDocumento1 paginaFigure 2: Physiological Responses To StressRaiyan KhanNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Structural Design and Optimization - Part IIDocumento448 pagineStructural Design and Optimization - Part IIFranco Bontempi100% (1)
- Preserving and Randomizing Data Responses in Web Application Using Differential PrivacyDocumento9 paginePreserving and Randomizing Data Responses in Web Application Using Differential PrivacyInternational Journal of Innovative Science and Research Technology100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Economic Order QuantityDocumento3 pagineEconomic Order QuantitySudhakar DoijadNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Behavior of Structure Under Blast LoadingDocumento32 pagineBehavior of Structure Under Blast Loadingramyashri inalaNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- 001-MBA-SPSS Applications - 10-06-2023Documento74 pagine001-MBA-SPSS Applications - 10-06-2023seyon sithamparanathanNessuna valutazione finora
- Principles of Gas Chromatography 2Documento12 paginePrinciples of Gas Chromatography 2Enanahmed EnanNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Prime Number FactorizationDocumento10 paginePrime Number FactorizationedithaenriquezNessuna valutazione finora
- Effect of Salinity On Proteins in Some Wheat CultivarsDocumento9 pagineEffect of Salinity On Proteins in Some Wheat Cultivarsray m deraniaNessuna valutazione finora
- Teacher PPT - Scientific RevolutionDocumento13 pagineTeacher PPT - Scientific Revolutionapi-441776741Nessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- BMTC 132Documento16 pagineBMTC 132Deepak Chaudhary JaatNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- AN17825ADocumento8 pagineAN17825AJose M PeresNessuna valutazione finora
- How Do Bodies MoveDocumento28 pagineHow Do Bodies Movedeme2411Nessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Science July Assignment Grade 8Documento3 pagineScience July Assignment Grade 8G PNessuna valutazione finora
- A Simulation of Attempts To Influence Crowd Dynamics'Documento6 pagineA Simulation of Attempts To Influence Crowd Dynamics'KhairulNessuna valutazione finora
- Database Management Systems: Lecture - 5Documento37 pagineDatabase Management Systems: Lecture - 5harisNessuna valutazione finora
- Zott Business ModelDocumento25 pagineZott Business ModelNico LightNessuna valutazione finora
- Fascial Manipulation For Internal Dysfunctions FMIDDocumento8 pagineFascial Manipulation For Internal Dysfunctions FMIDdavidzhouNessuna valutazione finora
- ESPKey Tool Manual v1.0.0Documento36 pagineESPKey Tool Manual v1.0.0Jad HaddadNessuna valutazione finora
- Guidelines For Utility Impact Assessment For Local Roads in Developed Areas MME 2012 Cross-SectionDocumento81 pagineGuidelines For Utility Impact Assessment For Local Roads in Developed Areas MME 2012 Cross-Sectionirfan mohammedNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- C ValueDocumento2 pagineC ValuePadmanabh Shetty0% (1)
- Builders' Metalwork: Ci/Sfb 21.9 Xt6Documento32 pagineBuilders' Metalwork: Ci/Sfb 21.9 Xt6JC TsuiNessuna valutazione finora
- Total Phenolic and Flavonoid Contents of Srikaya (Annona Squamosa L.) Leaf Fermented ExtractsDocumento14 pagineTotal Phenolic and Flavonoid Contents of Srikaya (Annona Squamosa L.) Leaf Fermented ExtractsAhmad HidayahNessuna valutazione finora
- Force Vectors: Scalars and Vectors 2D and 3D Force SystemsDocumento20 pagineForce Vectors: Scalars and Vectors 2D and 3D Force Systemsdanaluca2753Nessuna valutazione finora
- Table and Graph CriteriaDocumento3 pagineTable and Graph Criteriaapi-271250844Nessuna valutazione finora
- The Equation of The Straight Line: y MX CDocumento6 pagineThe Equation of The Straight Line: y MX CMarc SugrueNessuna valutazione finora
- Andrew KC Chan (2003) - Observations From Excavations - A ReflectionDocumento19 pagineAndrew KC Chan (2003) - Observations From Excavations - A ReflectionMan Ho LamNessuna valutazione finora
- 03 VEX SpotDocumento2 pagine03 VEX SpottemamNessuna valutazione finora
- PHP Question AnswerDocumento20 paginePHP Question AnswerManish SharmaNessuna valutazione finora
- Activity 2 Resultant Vector by Graphical MethodDocumento2 pagineActivity 2 Resultant Vector by Graphical MethodRick Ignacio0% (1)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)