Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- 10 Herbs For Hair GrowthDocumento2 pagine10 Herbs For Hair GrowthElžbieta GliaudelytėNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Skeletal System-Lecture NotesDocumento9 pagineSkeletal System-Lecture Notesjcali06100% (5)
- QAGS 2e - Funkadelic Frankenstein On The Mean Streets of Monstertown PDFDocumento8 pagineQAGS 2e - Funkadelic Frankenstein On The Mean Streets of Monstertown PDFGon_1313100% (1)
- +homespun FunDocumento76 pagine+homespun FunAna-Maria Ignat0% (1)
- Science Class 4 HabitatsDocumento6 pagineScience Class 4 HabitatsCatherine JeaneNessuna valutazione finora
- (Adrian Franklin) Animals and Modern Cultures A S (B-Ok - CC) PDFDocumento205 pagine(Adrian Franklin) Animals and Modern Cultures A S (B-Ok - CC) PDFBrenoVilelaNessuna valutazione finora
- Macpherson Et Al, 2013 Dogs, Zoonoses and PHDocumento288 pagineMacpherson Et Al, 2013 Dogs, Zoonoses and PHNath Bixo100% (1)
- Gato Manos ArribaDocumento6 pagineGato Manos ArribaLaura Portilla100% (1)
- Vargas Et Al 2016 Frequency of Anti Toxocara SPPDocumento7 pagineVargas Et Al 2016 Frequency of Anti Toxocara SPPNath BixoNessuna valutazione finora
- Jack Canfield THE POWER OF FOCUS PDFDocumento169 pagineJack Canfield THE POWER OF FOCUS PDFJohn Arango83% (12)
- Carter y Johnson 2012 Brucella Canis A Threat To Canine and Human HealthDocumento2 pagineCarter y Johnson 2012 Brucella Canis A Threat To Canine and Human HealthNath BixoNessuna valutazione finora
- Ficht 2010, Brucella TaxonomyDocumento11 pagineFicht 2010, Brucella TaxonomyNath BixoNessuna valutazione finora
- Global Burden of Canine Rabies PDFDocumento20 pagineGlobal Burden of Canine Rabies PDFNath BixoNessuna valutazione finora
- Glover, CP T2v Vaccine Protects Puppies With Maternal Antibodies To CPV When Challenged With CPV2b, 2012Documento8 pagineGlover, CP T2v Vaccine Protects Puppies With Maternal Antibodies To CPV When Challenged With CPV2b, 2012Nath BixoNessuna valutazione finora
- Genotyping of Canine Parvovirus in Western MexicoDocumento5 pagineGenotyping of Canine Parvovirus in Western MexicoNath BixoNessuna valutazione finora
- Innate Immune Responses To DNA VirusesDocumento7 pagineInnate Immune Responses To DNA VirusesNath BixoNessuna valutazione finora
- Vijay, Innate Immune Sensing of DNa Viruses 2011Documento21 pagineVijay, Innate Immune Sensing of DNa Viruses 2011Nath BixoNessuna valutazione finora
- Puentes, Eliopulos. Isolation and Characterization of Canine Parvovirus Type 2c (Cpv-2c) From Symptomatic - 2012Documento5 paginePuentes, Eliopulos. Isolation and Characterization of Canine Parvovirus Type 2c (Cpv-2c) From Symptomatic - 2012Nath BixoNessuna valutazione finora
- Tsugawa, Hoshino. Whole Genome Sequence and Phylogenic Analyses Reveals Human Rotavirus G3P 3 Strain Ro1845 and HCR3A Are Examples of Direct Virion Transmission of Canine Feline Rotaviruses to Humans. 2008Documento10 pagineTsugawa, Hoshino. Whole Genome Sequence and Phylogenic Analyses Reveals Human Rotavirus G3P 3 Strain Ro1845 and HCR3A Are Examples of Direct Virion Transmission of Canine Feline Rotaviruses to Humans. 2008Nath BixoNessuna valutazione finora
- Vivek Et Al 2013 Molecular Epidemiology of Canine Parvovirus in Southern IndiaDocumento6 pagineVivek Et Al 2013 Molecular Epidemiology of Canine Parvovirus in Southern IndiaNath BixoNessuna valutazione finora
- Horzinek, Vaccine Use and Disease Prevalece in Dogs and CatsDocumento7 pagineHorzinek, Vaccine Use and Disease Prevalece in Dogs and CatsNath BixoNessuna valutazione finora
- Involvement of A Non-Human Sialic Acid in Human CancerDocumento13 pagineInvolvement of A Non-Human Sialic Acid in Human CancerNath BixoNessuna valutazione finora
- Canine and Feline Parvoviruses Can Use Human or Feline Transferrin Receptors To Bind, Enter, and Infect CellsDocumento8 pagineCanine and Feline Parvoviruses Can Use Human or Feline Transferrin Receptors To Bind, Enter, and Infect CellsNath BixoNessuna valutazione finora
- Chappuis, Neonatal Immunity and Immunisation in Early Age. Lesons From Veterinary MedicineDocumento5 pagineChappuis, Neonatal Immunity and Immunisation in Early Age. Lesons From Veterinary MedicineNath BixoNessuna valutazione finora
- High Rate of Viral Evolution AssociatedDocumento7 pagineHigh Rate of Viral Evolution AssociatedNath BixoNessuna valutazione finora
- Journal of Virological MethodsDocumento2 pagineJournal of Virological MethodsNath BixoNessuna valutazione finora
- Pratelli, Cavalli Et Al, CP Vaccination Comparison of Neutralizing Antibody Responses in Pup After Inpcullation With CPV2 y 2b Vaccine VVMDocumento4 paginePratelli, Cavalli Et Al, CP Vaccination Comparison of Neutralizing Antibody Responses in Pup After Inpcullation With CPV2 y 2b Vaccine VVMNath BixoNessuna valutazione finora
- Pathways of Cell Infection by ParvovirusesDocumento6 paginePathways of Cell Infection by ParvovirusesNath BixoNessuna valutazione finora
- Wu Fang Tzy 2012 Putative Canine Origin of Rotavirus Strain Detected in A Child With Diarrhea.Documento4 pagineWu Fang Tzy 2012 Putative Canine Origin of Rotavirus Strain Detected in A Child With Diarrhea.Nath BixoNessuna valutazione finora
- Evidence For Immunisation Failure in Vaccinated Adult Dogs With CP Type 2cDocumento6 pagineEvidence For Immunisation Failure in Vaccinated Adult Dogs With CP Type 2cNath BixoNessuna valutazione finora
- Decaro, Elia - Real-Time PCR of CP T2 in Feces. 2004Documento10 pagineDecaro, Elia - Real-Time PCR of CP T2 in Feces. 2004Nath BixoNessuna valutazione finora
- Martella, Bányai, Zoonotic Aspects of Rotaviruses. 2010Documento10 pagineMartella, Bányai, Zoonotic Aspects of Rotaviruses. 2010Nath BixoNessuna valutazione finora
- NIH Public AccessDocumento18 pagineNIH Public AccessNath BixoNessuna valutazione finora
- Langeveld, Casal (1994) First Peptide Vaccine Providing Protection Against Viral Infection in The Target Animal. Journal of VirologyDocumento8 pagineLangeveld, Casal (1994) First Peptide Vaccine Providing Protection Against Viral Infection in The Target Animal. Journal of VirologyNath BixoNessuna valutazione finora
- De Grazia, Martella. Canine Origina G3P Rotavirus Strain in Child With Acute GastroenteritisDocumento3 pagineDe Grazia, Martella. Canine Origina G3P Rotavirus Strain in Child With Acute GastroenteritisNath BixoNessuna valutazione finora
- Kyu, Song, Jung, Geneticcharacterization of Canine Rotavirus Isolated From Puppy in Korea and Experimetal Reproduction Desease. 2007Documento7 pagineKyu, Song, Jung, Geneticcharacterization of Canine Rotavirus Isolated From Puppy in Korea and Experimetal Reproduction Desease. 2007Nath BixoNessuna valutazione finora
- 1.ordinary DaysDocumento4 pagine1.ordinary DaysJunan100% (1)
- King Marangle v1.0Documento21 pagineKing Marangle v1.0Shawn IsaacNessuna valutazione finora
- Plants For Food and Fibre WebquestDocumento2 paginePlants For Food and Fibre Webquestapi-237961942100% (1)
- AustraliaDocumento4 pagineAustraliaOana PopaNessuna valutazione finora
- Prehistoric Paleolithic and Neolithic MyDocumento5 paginePrehistoric Paleolithic and Neolithic MyonrNessuna valutazione finora
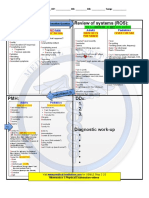
- CS Blue Sheet Mnemonics - USMLE Step 2 CS - WWW - MedicalDocumento1 paginaCS Blue Sheet Mnemonics - USMLE Step 2 CS - WWW - MedicalMaya Seegers100% (1)
- Try Out 1920Documento11 pagineTry Out 1920laras listianiNessuna valutazione finora
- Journal Reading Rhinitis and PregnancyDocumento29 pagineJournal Reading Rhinitis and PregnancyDestiWindaUtamiNessuna valutazione finora
- Organic Manifesto: How Organic Farming Can Heal Our Planet, Feed The World, and Keep Us SafeDocumento19 pagineOrganic Manifesto: How Organic Farming Can Heal Our Planet, Feed The World, and Keep Us SafekenleyneufeldNessuna valutazione finora
- Tenka Tells A StoryDocumento5 pagineTenka Tells A StoryshekereafricaNessuna valutazione finora
- 2021 SSPT Sample Questions Answer SheetsDocumento84 pagine2021 SSPT Sample Questions Answer SheetsManikandan BalakrishnanNessuna valutazione finora
- Pacesetter Starter WB Páginas 20 26Documento7 paginePacesetter Starter WB Páginas 20 26Luis CedricNessuna valutazione finora
- Good Home Pet Adoptions, Inc. Cat Foster Home AgreementDocumento6 pagineGood Home Pet Adoptions, Inc. Cat Foster Home AgreementJustin CollierNessuna valutazione finora
- How To Do Wildlife Conservation PDFDocumento4 pagineHow To Do Wildlife Conservation PDFNitinNessuna valutazione finora
- The Philippine Red CrossDocumento3 pagineThe Philippine Red CrossKeith Gretchen Lumibao CorumNessuna valutazione finora
- Lesson PlanDocumento12 pagineLesson PlanSagita JojobaNessuna valutazione finora
- Fleming Et Al 2009Documento27 pagineFleming Et Al 2009Simon Garth PurserNessuna valutazione finora
- Bersalona, Carmelita B.Documento6 pagineBersalona, Carmelita B.Mr. RightNessuna valutazione finora
- The Ant and The DoveDocumento6 pagineThe Ant and The DoveFaisal ArzaniNessuna valutazione finora
- Where The Red Fern Grows ReportDocumento3 pagineWhere The Red Fern Grows ReportDivine TrinitySchoolNessuna valutazione finora
- Reading 5Documento79 pagineReading 5dangnganha159100% (2)
- Short CasesDocumento4 pagineShort CasesnasanbuyanNessuna valutazione finora
- The Saddle Room MenuDocumento11 pagineThe Saddle Room MenuManzoor RiazNessuna valutazione finora