Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Pregnancy ProtocolDocumento7 paginePregnancy Protocolpiano543Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- 12 in 12Documento1 pagina12 in 12piano543Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Racial Disparities in Postpartum Pain Management.4Documento7 pagineRacial Disparities in Postpartum Pain Management.4piano543Nessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- 06 SMI Nifedipine Algorithm July 2017Documento1 pagina06 SMI Nifedipine Algorithm July 2017piano543Nessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- 03 SMI Eclampsia Checklist July 2017Documento1 pagina03 SMI Eclampsia Checklist July 2017piano543100% (1)
- PAA Neighborhood Survey 2016Documento11 paginePAA Neighborhood Survey 2016piano543Nessuna valutazione finora
- Mock Oral Series LegendDocumento1 paginaMock Oral Series Legendpiano543Nessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Ultrasound BasicsDocumento2 pagineUltrasound Basicspiano543Nessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Name of My Service: Please Call (555) 555-1234 or Text (555) 555-5678Documento2 pagineName of My Service: Please Call (555) 555-1234 or Text (555) 555-5678piano543Nessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Oral Board Crib Memory PDFDocumento10 pagineOral Board Crib Memory PDFpiano543Nessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Anesthesia Drugs Quick Reference Low ResDocumento6 pagineAnesthesia Drugs Quick Reference Low Respiano543Nessuna valutazione finora
- Mock Oral Exams IDocumento28 pagineMock Oral Exams Ipiano543Nessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- FA Mnemonics JSDocumento7 pagineFA Mnemonics JSpiano543Nessuna valutazione finora
- Aldrete Discharge ScoresDocumento1 paginaAldrete Discharge Scorespiano543Nessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Remote Access Portal User Guide SSLVPNDocumento11 pagineRemote Access Portal User Guide SSLVPNpiano543Nessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Medtext 2007 A-Type QuestionsDocumento16 pagineMedtext 2007 A-Type Questionspiano543Nessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- 1996 Ite ExamDocumento72 pagine1996 Ite Exampiano543Nessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Sia Breathe MeDocumento7 pagineSia Breathe MeEnrico VolpatoNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Forensic 5 Powerpoint Week1 2Documento39 pagineForensic 5 Powerpoint Week1 2Jayson BianidaNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
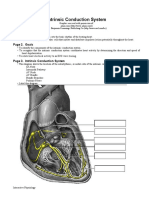
- Intrinsic Conduction System: Page 1. IntroductionDocumento5 pagineIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Cardiovascular Physiology Concepts - 2nd EditionDocumento257 pagineCardiovascular Physiology Concepts - 2nd EditionAbel GarcíaNessuna valutazione finora
- H020 02 Mark Scheme Dec 15Documento18 pagineH020 02 Mark Scheme Dec 15ny6k26sbx9Nessuna valutazione finora
- Jugular Venous Pressure: Syed Farrukh UmairDocumento30 pagineJugular Venous Pressure: Syed Farrukh UmairsfumairNessuna valutazione finora
- Unit II (B) Intra-Aortic Balloon Pump Counter PulsationDocumento24 pagineUnit II (B) Intra-Aortic Balloon Pump Counter PulsationUmme HabibaNessuna valutazione finora
- Circulatory and Respiratory Systems - Module 3Documento47 pagineCirculatory and Respiratory Systems - Module 3CaityNessuna valutazione finora
- Pacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Documento46 paginePacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Zahangir Kabir AshikNessuna valutazione finora
- Guidelines TAVI TAVRDocumento15 pagineGuidelines TAVI TAVRRossellaDisalvo100% (1)
- PP 1 Biologi - Tingkatan 5 - Kertas 1Documento22 paginePP 1 Biologi - Tingkatan 5 - Kertas 1hairulNessuna valutazione finora
- Echocardiography Function Guiline Image 추가Documento105 pagineEchocardiography Function Guiline Image 추가stoicea catalin100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- June 2008 QP - Paper 1 CIE Biology A-LevelDocumento20 pagineJune 2008 QP - Paper 1 CIE Biology A-LevelDamien SibandaNessuna valutazione finora
- Cardiovascular System PDFDocumento71 pagineCardiovascular System PDFramadanNessuna valutazione finora
- Heart Structure and FunctionsDocumento3 pagineHeart Structure and FunctionsChristella KateNessuna valutazione finora
- Notes: Student Book 1Documento115 pagineNotes: Student Book 1Farah AwadNessuna valutazione finora
- Biology Form 2 NotesDocumento80 pagineBiology Form 2 NotesLutern RayNessuna valutazione finora
- Complete Heart BlockDocumento13 pagineComplete Heart BlockSubhranil MaityNessuna valutazione finora
- Chapter18 TheCardiovascularSystem TheHeartDocumento7 pagineChapter18 TheCardiovascularSystem TheHeartChelsea CunninghamNessuna valutazione finora
- The Cardiac Electrical System and How The HeartDocumento26 pagineThe Cardiac Electrical System and How The HeartZoe Jisel LuzadasNessuna valutazione finora
- Cardiovascular Notes - All in One FileDocumento299 pagineCardiovascular Notes - All in One FileHasan DiabNessuna valutazione finora
- Unit 3Documento25 pagineUnit 3senthilNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Answers To Eocqs: Notes About Mark SchemesDocumento3 pagineAnswers To Eocqs: Notes About Mark SchemesAayush Gauchan0% (1)
- PacemakersDocumento8 paginePacemakersVIVEK Kumar Prajapati 72Nessuna valutazione finora
- Hepatic Vein FlowDocumento14 pagineHepatic Vein FlowJORGENessuna valutazione finora
- 2.02 Gross Anatomy Trans - HeartDocumento15 pagine2.02 Gross Anatomy Trans - HeartElma Gonzales100% (1)
- Science Primary 5 Second Term 2015SciencePrimary5secondTERM2015مذكرة علوم لغات الصف الخامس الابتدائي الترم الثاني لغات 2015Documento26 pagineScience Primary 5 Second Term 2015SciencePrimary5secondTERM2015مذكرة علوم لغات الصف الخامس الابتدائي الترم الثاني لغات 2015rabei91% (22)
- Hkcee Biology - 4.6 Transport in Humans - P.1Documento13 pagineHkcee Biology - 4.6 Transport in Humans - P.1irisyyy27Nessuna valutazione finora
- 8th Sem ProjectDocumento29 pagine8th Sem ProjectRashmi B ReddyNessuna valutazione finora
- Atrial Systole: The End of DiastoleDocumento9 pagineAtrial Systole: The End of DiastoleSophia MahboobNessuna valutazione finora
- Angina PectorisDocumento20 pagineAngina PectorisJyoti singhNessuna valutazione finora
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)