Potrebbero piacerti anche
- Elements of Short Story WORKBOOKDocumento26 pagineElements of Short Story WORKBOOKDavid Velez Gonzalez100% (2)
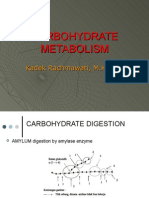
- Carbohydrate MetabolismDocumento38 pagineCarbohydrate Metabolismwidya nurrohmanNessuna valutazione finora
- Alternative ADHD TreatmentDocumento3 pagineAlternative ADHD TreatmentCindy VanegasNessuna valutazione finora
- Indian Oil Corporation LTD Guwahati RefineryDocumento27 pagineIndian Oil Corporation LTD Guwahati Refineryelectram67% (6)
- HBR's 10 Must Reads on Strategy for Healthcare (featuring articles by Michael E. Porter and Thomas H. Lee, MD)Da EverandHBR's 10 Must Reads on Strategy for Healthcare (featuring articles by Michael E. Porter and Thomas H. Lee, MD)Valutazione: 4 su 5 stelle4/5 (3)
- Deloitte IT Governance SurveyDocumento20 pagineDeloitte IT Governance Surveymrehan2k2Nessuna valutazione finora
- Case Study ResearchDocumento20 pagineCase Study ResearchManish PuttyahNessuna valutazione finora
- Lean Done Right: Achieve and Maintain Reform in Your Healthcare OrganizationDa EverandLean Done Right: Achieve and Maintain Reform in Your Healthcare OrganizationNessuna valutazione finora
- Making the Healthcare Shift: The Transformation to Consumer-CentricityDa EverandMaking the Healthcare Shift: The Transformation to Consumer-CentricityNessuna valutazione finora
- Thesis Topics On Health InsuranceDocumento7 pagineThesis Topics On Health Insuranceamynelsonannarbor100% (2)
- Research Papers Are Written in What Point of ViewDocumento8 pagineResearch Papers Are Written in What Point of ViewafnkceovfqcvwpNessuna valutazione finora
- Research Paper On Health CareDocumento4 pagineResearch Paper On Health CareafeaynwqzNessuna valutazione finora
- Healthcare Economic Research Paper TopicsDocumento4 pagineHealthcare Economic Research Paper Topicsafmcsvatc100% (1)
- Mba Thesis Topics in Health CareDocumento8 pagineMba Thesis Topics in Health Caresuejonessalem100% (2)
- Sme Dissertation TopicsDocumento6 pagineSme Dissertation TopicsPaperWritingServicesReviewsUK100% (1)
- Clarka 1140432 - Literature ReviewDocumento5 pagineClarka 1140432 - Literature Reviewapi-610041865Nessuna valutazione finora
- Health Insurance ThesisDocumento5 pagineHealth Insurance Thesisginabuckboston100% (2)
- Research Paper On Health Care PDFDocumento6 pagineResearch Paper On Health Care PDFefkm3yz9100% (1)
- Health Insurance Thesis StatementDocumento7 pagineHealth Insurance Thesis Statementbk32hdq7100% (2)
- Term Paper On Health Care ReformDocumento6 pagineTerm Paper On Health Care Reformdrnpguwgf100% (1)
- Good Health Care Topics For Research PaperDocumento4 pagineGood Health Care Topics For Research Paperlzpyreqhf100% (1)
- Research Paper Topics On Health InsuranceDocumento5 pagineResearch Paper Topics On Health Insurancevguneqrhf100% (1)
- Research Paper Topics Health Care AdministrationDocumento7 pagineResearch Paper Topics Health Care AdministrationafnjobmwsvoamuNessuna valutazione finora
- Health Care Management Research Paper TopicsDocumento9 pagineHealth Care Management Research Paper Topicscapz4pp5100% (1)
- Health Insurance Dissertation TopicsDocumento6 pagineHealth Insurance Dissertation TopicsPapersWritingServiceCanada100% (1)
- Term Paper On Affordable Care ActDocumento4 pagineTerm Paper On Affordable Care Actc5p8vze7100% (1)
- Center For Global Development: EssayDocumento6 pagineCenter For Global Development: EssayJosh2002Nessuna valutazione finora
- Health Research Paper TopicsDocumento5 pagineHealth Research Paper Topicsgvw6y2hv100% (1)
- Research Paper Topics For Health ClassDocumento6 pagineResearch Paper Topics For Health Classgz8te40w100% (1)
- Research Paper On Health Care CostsDocumento6 pagineResearch Paper On Health Care Costsgw1nm9nb100% (1)
- Research Paper On Health Care ManagementDocumento7 pagineResearch Paper On Health Care Managementrsbptyplg100% (1)
- Health Economics PHD Thesis TopicsDocumento5 pagineHealth Economics PHD Thesis TopicsBuySchoolPapersSingapore100% (1)
- Dissertation Topics in Healthcare ManagementDocumento6 pagineDissertation Topics in Healthcare ManagementWebsiteThatWillWriteAPaperForYouOmaha100% (1)
- Medical Law Dissertation TitlesDocumento4 pagineMedical Law Dissertation TitlesBuyThesisPaperSingapore100% (1)
- Better Outcomes Lower Costs FSG&GIH Spring 2012Documento18 pagineBetter Outcomes Lower Costs FSG&GIH Spring 2012iggybauNessuna valutazione finora
- Thesis Statement Healthcare ReformDocumento8 pagineThesis Statement Healthcare Reformashleycornettneworleans100% (2)
- Payment Reform Work Group Report 2-18-11 - FinalDocumento65 paginePayment Reform Work Group Report 2-18-11 - FinalRhett SemonesNessuna valutazione finora
- Health Topic Ideas For Research PapersDocumento6 pagineHealth Topic Ideas For Research Papersniisexgkf100% (1)
- Research Paper Topics For Healthcare AdministrationDocumento7 pagineResearch Paper Topics For Healthcare Administrationgw0q12dx100% (1)
- Medical Thesis IdeasDocumento6 pagineMedical Thesis Ideastkxajlhld100% (1)
- Dissertation Global HealthDocumento7 pagineDissertation Global HealthBuyingCollegePapersPittsburgh100% (1)
- Public Health Master Thesis TopicsDocumento5 paginePublic Health Master Thesis Topicsfjcsp27e100% (2)
- Healthcare Management Thesis TopicsDocumento6 pagineHealthcare Management Thesis TopicsBecky Goins100% (2)
- Research Paper Topics For Healthcare ManagementDocumento4 pagineResearch Paper Topics For Healthcare ManagementaflbqtfvhNessuna valutazione finora
- Thesis Topics in Community HealthDocumento8 pagineThesis Topics in Community Healthalyssadennischarleston100% (2)
- Bend the Healthcare Trend: How Consumer-Driven Health & Wellness Plans Lower Insurance CostsDa EverandBend the Healthcare Trend: How Consumer-Driven Health & Wellness Plans Lower Insurance CostsNessuna valutazione finora
- Ensayos Sobre La Revolución IndustrialDocumento13 pagineEnsayos Sobre La Revolución Industrialg69pcj6h100% (1)
- Thesis Health InsuranceDocumento5 pagineThesis Health Insuranceamandadetwilerpeoria100% (2)
- Research Paper On Interest GroupsDocumento4 pagineResearch Paper On Interest Groupsgrgdazukg100% (1)
- Thesis Health EducationDocumento5 pagineThesis Health Educationcoawokugg100% (2)
- Research Paper On Civil UnionsDocumento9 pagineResearch Paper On Civil Unionstwdhopwgf100% (1)
- Thesis Topics in Hospital AdministrationDocumento5 pagineThesis Topics in Hospital Administrationfc2g5tmd100% (1)
- Health Insurance Research Paper ThesisDocumento7 pagineHealth Insurance Research Paper Thesiskatieellismanchester100% (1)
- Research Paper Health Care ReformDocumento4 pagineResearch Paper Health Care Reformsjcuwurif100% (1)
- Research Paper On Affordable Health CareDocumento6 pagineResearch Paper On Affordable Health Caregz8zw71w100% (1)
- Medicare ThesisDocumento5 pagineMedicare Thesisnicolekatholoverlandpark100% (2)
- Thesis Topics Community MedicineDocumento7 pagineThesis Topics Community MedicineMonique Carr100% (1)
- Individual and Organizational Ethics: Social ResponsibilityDocumento4 pagineIndividual and Organizational Ethics: Social ResponsibilityJulianaNessuna valutazione finora
- Us Healthcare Research Paper TopicsDocumento6 pagineUs Healthcare Research Paper Topicsaflbasnka100% (1)
- Nursing Research Paper GuidelinesDocumento9 pagineNursing Research Paper Guidelinesaflbmmddd100% (1)
- 2 Structural Frame WorksheetDocumento3 pagine2 Structural Frame Worksheetapi-654727753Nessuna valutazione finora
- Dissertation On Care HomesDocumento4 pagineDissertation On Care HomesBuyingCollegePapersCanada100% (1)
- Dissertation Examples Health Social CareDocumento6 pagineDissertation Examples Health Social CarePaperWriterServiceUK100% (1)
- Healthcare Thesis StatementDocumento5 pagineHealthcare Thesis Statementbethjohnsonomaha100% (2)
- Hospital Administration Research PapersDocumento6 pagineHospital Administration Research Papersafmcbmoag100% (1)
- A Good Thesis Statement For Health Care ReformDocumento5 pagineA Good Thesis Statement For Health Care Reformfc2b5myj100% (2)
- Six Sigma FordDocumento8 pagineSix Sigma FordMilagros Karina Calapuja QuispeNessuna valutazione finora
- Geometrica Builds Iso 9001Documento7 pagineGeometrica Builds Iso 9001Milagros Karina Calapuja QuispeNessuna valutazione finora
- Change Ahead: Standards OutlookDocumento3 pagineChange Ahead: Standards OutlookMilagros Karina Calapuja QuispeNessuna valutazione finora
- Opinion: Healthcare's Next Big HIT?Documento2 pagineOpinion: Healthcare's Next Big HIT?Milagros Karina Calapuja QuispeNessuna valutazione finora
- Service Manual: Digital Laser Copier/ Digital Multifunctional SystemDocumento132 pagineService Manual: Digital Laser Copier/ Digital Multifunctional SystemViktor FehlerNessuna valutazione finora
- Mewaruniversity PH DDocumento4 pagineMewaruniversity PH Dpramoddutta100% (1)
- Statistics Mid-Term Exam - February 2023Documento18 pagineStatistics Mid-Term Exam - February 2023Delse PeterNessuna valutazione finora
- Dario Great Wall of China Lesson PlanDocumento3 pagineDario Great Wall of China Lesson Planapi-297914033Nessuna valutazione finora
- Data Gathering Advantage and DisadvantageDocumento4 pagineData Gathering Advantage and DisadvantageJuan VeronNessuna valutazione finora
- Aavit 5 ADocumento113 pagineAavit 5 AAnonymous ok5UankNessuna valutazione finora
- Recurrent Neural Processes: Preprint. Under ReviewDocumento12 pagineRecurrent Neural Processes: Preprint. Under Reviewgheorghe garduNessuna valutazione finora
- v53nS5 Bio Anthro SupplementDocumento272 paginev53nS5 Bio Anthro SupplementJean-FrançoisVéranNessuna valutazione finora
- Jurutera August 2014Documento28 pagineJurutera August 2014Edison LimNessuna valutazione finora
- Calnetix BrochureDocumento6 pagineCalnetix Brochuresh_saraydin3949Nessuna valutazione finora
- Q1. Read The Passage Below and Answer The Questions That FollowDocumento3 pagineQ1. Read The Passage Below and Answer The Questions That FollowAryan KananiNessuna valutazione finora
- My Black BookDocumento5 pagineMy Black BookRiSHI KeSH GawaINessuna valutazione finora
- High School Kids Science Fiction Short StoriesDocumento5 pagineHigh School Kids Science Fiction Short StoriesHarshal bhardwaj100% (1)
- Family Day by Day - The Guide To A Successful Family LifeDocumento212 pagineFamily Day by Day - The Guide To A Successful Family Lifeprajya100% (3)
- Younified LevelupDocumento9 pagineYounified LevelupMitesh NagpalNessuna valutazione finora
- Health Indicators DemographyDocumento35 pagineHealth Indicators DemographyZoe RodriguezNessuna valutazione finora
- An Overview On Co-Operative Societies in BangladeshDocumento11 pagineAn Overview On Co-Operative Societies in BangladeshAlexander DeckerNessuna valutazione finora
- Case MC ColleaguesVsClientsDocumento2 pagineCase MC ColleaguesVsClientsSri Harsha50% (2)
- 11697415Documento514 pagine11697415Anonymous nC9gpUWPNessuna valutazione finora
- Photo-Realistic 3D Model Extraction From Camera Array CaptureDocumento11 paginePhoto-Realistic 3D Model Extraction From Camera Array CaptureJohn NaylorNessuna valutazione finora
- Accu MAX3000Documento2 pagineAccu MAX3000ynod70Nessuna valutazione finora
- The MES Performance Advantage Best of The Best Plants Use MESDocumento20 pagineThe MES Performance Advantage Best of The Best Plants Use MESNiraj KumarNessuna valutazione finora
- Viltam User Manual enDocumento13 pagineViltam User Manual enszol888Nessuna valutazione finora
- Review On Hand Gesture RecognitionDocumento5 pagineReview On Hand Gesture RecognitiondbpublicationsNessuna valutazione finora