Potrebbero piacerti anche
- Vista Hepatitis B Surface AntigenDocumento3 pagineVista Hepatitis B Surface Antigenadam parthen kaneNessuna valutazione finora
- Experiment 9 Hepatitis B Surface Antigen & Anti-Hepatitis B Surface Antigen Test (Hbsag & Anti-Hbsag Test)Documento3 pagineExperiment 9 Hepatitis B Surface Antigen & Anti-Hepatitis B Surface Antigen Test (Hbsag & Anti-Hbsag Test)Rod PasionNessuna valutazione finora
- One Step Anti-HIV (1&2) TestDocumento4 pagineOne Step Anti-HIV (1&2) TestGail Ibanez100% (1)
- HIV 1 2 Ab Rapid Test Cassette 1Documento5 pagineHIV 1 2 Ab Rapid Test Cassette 1Dewi LengkanawatiNessuna valutazione finora
- Leishcheck: Size: 137 X 218 MMDocumento4 pagineLeishcheck: Size: 137 X 218 MMMatibar RahmanNessuna valutazione finora
- HBsAb SerumDocumento2 pagineHBsAb SerumGENDRITZ100% (2)
- Laprak Imser HBsAGDocumento6 pagineLaprak Imser HBsAGashaarul97Nessuna valutazione finora
- Sagita Instrumen ElisaDocumento2 pagineSagita Instrumen ElisaReynaldiPandeirothNessuna valutazione finora
- Shera2HbsAg ConfDocumento8 pagineShera2HbsAg ConfSadia Sharmin NilimaNessuna valutazione finora
- Mybiosource: Covid-19 Igg/Igm Antibody Assay KitDocumento3 pagineMybiosource: Covid-19 Igg/Igm Antibody Assay KitMatibar RahmanNessuna valutazione finora
- Tuberculosis Igg/Igm Rapid Test Device (Serum/Plasma) : TH THDocumento6 pagineTuberculosis Igg/Igm Rapid Test Device (Serum/Plasma) : TH THSheilla DifaNessuna valutazione finora
- Serology Lecture NotesDocumento49 pagineSerology Lecture NotesPaul GasparNessuna valutazione finora
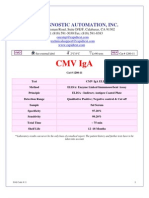
- CMV Ig A TorchDocumento5 pagineCMV Ig A TorchMigPNessuna valutazione finora
- Hivtest FileDocumento10 pagineHivtest FilemuradNessuna valutazione finora
- Immunology and Serology/ Blood Banking: Group 3Documento48 pagineImmunology and Serology/ Blood Banking: Group 3Kaycee Gretz LorescaNessuna valutazione finora
- Aminotransferaseserum Glutamic Oxaloacetic TransaminaseDocumento3 pagineAminotransferaseserum Glutamic Oxaloacetic Transaminaserose_almonteNessuna valutazione finora
- 3.1.1 HBsAg Testing (ELISA Method)Documento6 pagine3.1.1 HBsAg Testing (ELISA Method)Jeevan VkiNessuna valutazione finora
- 3.1.1 HBsAg Testing (ELISA Method)Documento6 pagine3.1.1 HBsAg Testing (ELISA Method)BALAJINessuna valutazione finora
- HBsAg 40 Tests Ing Rev. 07Documento2 pagineHBsAg 40 Tests Ing Rev. 07Mayra VallesNessuna valutazione finora
- HBSAG Rapid Test 2Documento6 pagineHBSAG Rapid Test 2Charlotte OhNessuna valutazione finora
- RAT Investigatory ProjectDocumento11 pagineRAT Investigatory ProjectanoopstudieNessuna valutazione finora
- Blood Grouping Reagents NBDocumento7 pagineBlood Grouping Reagents NBDominic EmerencianaNessuna valutazione finora
- 13fk10 Hav Igg-Igm (D) Ins (En) CeDocumento2 pagine13fk10 Hav Igg-Igm (D) Ins (En) CeCrcrjhjh RcrcjhjhNessuna valutazione finora
- Binax Product InsertDocumento96 pagineBinax Product Insertuber6791Nessuna valutazione finora
- H Pilory HecesDocumento2 pagineH Pilory HecesKarla SotoNessuna valutazione finora
- HCV Package InsertDocumento1 paginaHCV Package Insertgitadevistha23Nessuna valutazione finora
- Laboratory Procedure Manual: Hepatitis C Antibody / Hepatitis C Confirmatory Test (Anti-HCV) SerumDocumento25 pagineLaboratory Procedure Manual: Hepatitis C Antibody / Hepatitis C Confirmatory Test (Anti-HCV) SerumEi Ei ThetNessuna valutazione finora
- 708600Documento36 pagine708600claude_badrNessuna valutazione finora
- Hepa e Hepatitis-A-Antibody MetDocumento19 pagineHepa e Hepatitis-A-Antibody MetKrizia R. PingkeNessuna valutazione finora
- Instant-View: H. Pylori Serum Cassette TestDocumento2 pagineInstant-View: H. Pylori Serum Cassette TestGrace ValenciaNessuna valutazione finora
- Sars-Cov-2 Igg Elisa Kit (DEIASL019) : Product InformationDocumento6 pagineSars-Cov-2 Igg Elisa Kit (DEIASL019) : Product InformationТатьяна ИсаеваNessuna valutazione finora
- Advanced Diagnostic Immunohematology and Blood BankDocumento6 pagineAdvanced Diagnostic Immunohematology and Blood BankYaseen MohamnadNessuna valutazione finora
- Ifobt Single Package InsertDocumento4 pagineIfobt Single Package InsertDevi OktaviannyNessuna valutazione finora
- Hepc e Met Hep C RibaDocumento22 pagineHepc e Met Hep C Ribaعائش العموديNessuna valutazione finora
- Fecal Occult Blood TESTDocumento1 paginaFecal Occult Blood TESTdatitox67% (3)
- Rubella IgG 1301Z-WebDocumento6 pagineRubella IgG 1301Z-WebvolvoproNessuna valutazione finora
- 212 Antibody Detection Test Saline Method1Documento4 pagine212 Antibody Detection Test Saline Method1Alfreah Jean TambasenNessuna valutazione finora
- Laboratory Procedure Manual: Hepatitis B Core Antibody SerumDocumento14 pagineLaboratory Procedure Manual: Hepatitis B Core Antibody Serumakhmad ikhwanNessuna valutazione finora
- 2.5 Antibody ScreeningDocumento5 pagine2.5 Antibody ScreeningBALAJINessuna valutazione finora
- COBAS Elecsys HBsAgDocumento45 pagineCOBAS Elecsys HBsAgmeghnaNessuna valutazione finora
- Aso PDFDocumento2 pagineAso PDFMarwa_MakiKiNessuna valutazione finora
- Laboratory Procedure Manual: Hepatitis B Surface Antigen (Hbsag) Serum Auszyme MonoclonalDocumento13 pagineLaboratory Procedure Manual: Hepatitis B Surface Antigen (Hbsag) Serum Auszyme MonoclonalNika AndrianiNessuna valutazione finora
- IFU For SARS-CoV-2 Ab Diagnostic KitDocumento3 pagineIFU For SARS-CoV-2 Ab Diagnostic KitLeonel OjedaNessuna valutazione finora
- ASM Web Protocol Serology 062220 FINALDocumento11 pagineASM Web Protocol Serology 062220 FINALChristian Saldaña DonayreNessuna valutazione finora
- Hepbd J Met Hepatitis B Surface Antigen 508Documento18 pagineHepbd J Met Hepatitis B Surface Antigen 508Gom LinusNessuna valutazione finora
- Reszon Pi - Typhidot Rapid Igm 2011-01Documento2 pagineReszon Pi - Typhidot Rapid Igm 2011-01Harnadi WonogiriNessuna valutazione finora
- Can-Fte-260 - Free TestosteroneDocumento2 pagineCan-Fte-260 - Free TestosteronevijayaNessuna valutazione finora
- Widal TestDocumento11 pagineWidal TestlialestariNessuna valutazione finora
- Blood TypingDocumento2 pagineBlood TypingDahr ELNessuna valutazione finora
- Elisa: From A ZDocumento66 pagineElisa: From A ZMaria JozilynNessuna valutazione finora
- Hepb S D Met Hep B Surface AntibodyDocumento12 pagineHepb S D Met Hep B Surface AntibodyYulia NovitaNessuna valutazione finora
- Prueba Rapida de MononucleosisDocumento9 paginePrueba Rapida de MononucleosisValeria Ramirez MedinaNessuna valutazione finora
- ABO Forward and Reverse Tube MethodDocumento4 pagineABO Forward and Reverse Tube Method''Rochelle Mylene ﭢ Ygoña100% (1)
- Laporan Immun II LagiDocumento6 pagineLaporan Immun II Lagiashaarul97Nessuna valutazione finora
- HCV Hepatitis C Virus Antibody Rapid Test Immunofluorescence AssayDocumento2 pagineHCV Hepatitis C Virus Antibody Rapid Test Immunofluorescence AssayPhyo WaiNessuna valutazione finora
- Widal KitDocumento9 pagineWidal KitAhsan MustafaNessuna valutazione finora
- Sop For Abo GroupingDocumento10 pagineSop For Abo GroupingMohd Fekharudin Mahmud75% (4)
- Immuno ReportDocumento4 pagineImmuno ReportmechellesibandaNessuna valutazione finora
- Direct Antiglobulin TestDocumento4 pagineDirect Antiglobulin TestCattrainuhNessuna valutazione finora
- Immunohematology and Transfusion Medicine: A Case Study ApproachDa EverandImmunohematology and Transfusion Medicine: A Case Study ApproachNessuna valutazione finora
- Screening Who Instructions PDFDocumento72 pagineScreening Who Instructions PDFpbta punjabNessuna valutazione finora
- Article Wjpps 15465140481Documento12 pagineArticle Wjpps 15465140481Tech RajaNessuna valutazione finora
- Sample MCQsDocumento6 pagineSample MCQsRiyad AliNessuna valutazione finora
- HEPATITEDocumento49 pagineHEPATITEAeron TamayoNessuna valutazione finora
- Microbial CarcinogensDocumento33 pagineMicrobial CarcinogensJacob ThomasNessuna valutazione finora
- BBP Quiz N Answers 2Documento3 pagineBBP Quiz N Answers 2Kim KauerNessuna valutazione finora
- Bullets: "Victory Belongs To Those Who Are Most Persevering. Ad Majorem Dei Gloriam."Documento15 pagineBullets: "Victory Belongs To Those Who Are Most Persevering. Ad Majorem Dei Gloriam."Jhaylord mendozaNessuna valutazione finora
- Liver Function Test Liver Function Test Liver Function Test Liver Function TestDocumento2 pagineLiver Function Test Liver Function Test Liver Function Test Liver Function TestJ KNessuna valutazione finora
- Dr.T.V.Rao MD Dr.T.V.Rao MDDocumento108 pagineDr.T.V.Rao MD Dr.T.V.Rao MDprithviraj_tarafdarNessuna valutazione finora
- 4.daftar PustakaDocumento8 pagine4.daftar PustakaTsania MahiraNessuna valutazione finora
- Hepatitis C SlidesDocumento51 pagineHepatitis C SlidesChukwu NedumNessuna valutazione finora
- PHRI Mod 6Documento62 paginePHRI Mod 6mostey mosteyNessuna valutazione finora
- GonorrheaDocumento22 pagineGonorrheaSharah Londonio100% (1)
- 77 PAG LINKS-Danni-Vaccini PDFDocumento77 pagine77 PAG LINKS-Danni-Vaccini PDFAntonio MartiniNessuna valutazione finora
- Gashu Afework 23Documento88 pagineGashu Afework 23Alemayehu KebedeNessuna valutazione finora
- Infection in Pregnancy PDFDocumento39 pagineInfection in Pregnancy PDFsimmyvashisht100% (1)
- Reviews: Viral Hepatitis and PregnancyDocumento15 pagineReviews: Viral Hepatitis and PregnancyRANINessuna valutazione finora
- 2022 Communicable Disease Reference Guide For SchoolsDocumento118 pagine2022 Communicable Disease Reference Guide For Schoolsmohan s vNessuna valutazione finora
- Sample Chapter: Miscellaneous VirusesDocumento7 pagineSample Chapter: Miscellaneous VirusesskNessuna valutazione finora
- Frequently Used Medical AbbreviationsDocumento10 pagineFrequently Used Medical AbbreviationsdunareagalatiNessuna valutazione finora
- By: Hasan Suleiman Artem LorensDocumento35 pagineBy: Hasan Suleiman Artem LorenssgolbariNessuna valutazione finora
- First Aid PDFDocumento100 pagineFirst Aid PDFBettyblazetech100% (3)
- Git MRCGP 2015Documento170 pagineGit MRCGP 2015AlexandraOsmanNessuna valutazione finora
- Mock Outbreak Exercise: M. Serra Biol 2420 Lab Report 11 Student NameDocumento3 pagineMock Outbreak Exercise: M. Serra Biol 2420 Lab Report 11 Student NameDennis MuthusiNessuna valutazione finora
- Cirrhosis Hepatis 1Documento48 pagineCirrhosis Hepatis 1Muhammad RivaileNessuna valutazione finora
- PMLS - Definition of Curriculum and Overview of CoursesDocumento5 paginePMLS - Definition of Curriculum and Overview of CoursesVine OrtegaNessuna valutazione finora
- Premera Preventative Benefits PDFDocumento5 paginePremera Preventative Benefits PDFlindytindylindtNessuna valutazione finora
- Welcome To Addis Guide May 2010 - 0Documento95 pagineWelcome To Addis Guide May 2010 - 0fitsumsegedNessuna valutazione finora
- A Review On Ayurvedic Medicinal Herbs As Remedial Perspective For COVID-19Documento21 pagineA Review On Ayurvedic Medicinal Herbs As Remedial Perspective For COVID-19Prabhat KcNessuna valutazione finora
- GuidelinesDocumento151 pagineGuidelinesM. A.V.Nessuna valutazione finora