Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Efektifitas Terapi Massage Dengan Terapi Mandi Air Hangat TerhadapDocumento8 pagineEfektifitas Terapi Massage Dengan Terapi Mandi Air Hangat TerhadapAlfi Rohmatus SholihahNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Pengaruh Senam LansiaDocumento7 paginePengaruh Senam LansiaAlfi Rohmatus SholihahNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Terapi Musik KeroncongDocumento8 pagineTerapi Musik KeroncongAlfi Rohmatus SholihahNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- S G Brain With People Ho Have Parkinson'S Disease: Anna Shaw, Oregon, U.S.ADocumento4 pagineS G Brain With People Ho Have Parkinson'S Disease: Anna Shaw, Oregon, U.S.AAlfi Rohmatus SholihahNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Organisational Behaviour PDFDocumento129 pagineOrganisational Behaviour PDFHemant GuptaNessuna valutazione finora
- GA Classic Qualification SpecificationDocumento10 pagineGA Classic Qualification SpecificationThomasNessuna valutazione finora
- Didactic Unit Simple Present Tense ReviewDocumento3 pagineDidactic Unit Simple Present Tense ReviewEmersdavidNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- PIT-AR2022 InsidePages NewDocumento54 paginePIT-AR2022 InsidePages NewMaria Francisca SarinoNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- English Balbharati STD 1 PDFDocumento86 pagineEnglish Balbharati STD 1 PDFSwapnil C100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Final Superintendent Recommendation 2023Documento30 pagineFinal Superintendent Recommendation 2023ABC Action NewsNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Lesson Plan: Activity Activity 1: Warm-UpDocumento3 pagineLesson Plan: Activity Activity 1: Warm-UpSorina-Andrada IonNessuna valutazione finora
- Planning History Assignment-1: Book ReviewDocumento7 paginePlanning History Assignment-1: Book ReviewAditya KaranNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Louisa May Alcott Little Women Websters Thesaurus Edition 2006Documento658 pagineLouisa May Alcott Little Women Websters Thesaurus Edition 2006Alexander León Vega80% (5)
- My HanumanDocumento70 pagineMy Hanumanrajeshlodi100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Short Term Studentship 2021 Program Details and Guide For StudentsDocumento13 pagineShort Term Studentship 2021 Program Details and Guide For StudentsPrincy paulrajNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Grade 9 English Q2 Ws 3 4Documento9 pagineGrade 9 English Q2 Ws 3 4Jeremias MalbasNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Entrepreneural Ventrures - Sample Assignment 1Documento15 pagineEntrepreneural Ventrures - Sample Assignment 1Owais JunaidNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Pinpdf Com 91 Colour Prediction Trick 91 ClubDocumento3 paginePinpdf Com 91 Colour Prediction Trick 91 Clubsaimkhan8871340% (1)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Modern ScotsDocumento266 pagineModern ScotsLuis ARJOL PUEYONessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Test Manual: English ComprehensionDocumento9 pagineTest Manual: English ComprehensionAnonymous EU0KgOEPNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
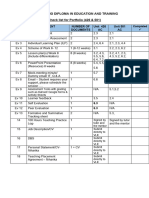
- Checklist For Portfolio Evidence (426 & 501) (Final)Documento1 paginaChecklist For Portfolio Evidence (426 & 501) (Final)undan.uk3234Nessuna valutazione finora
- Carnap, R. (1934) - On The Character of Philosophical Problems. Philosophy of Science, Vol. 1, No. 1Documento16 pagineCarnap, R. (1934) - On The Character of Philosophical Problems. Philosophy of Science, Vol. 1, No. 1Dúber CelisNessuna valutazione finora
- Laser Coaching: A Condensed 360 Coaching Experience To Increase Your Leaders' Confidence and ImpactDocumento3 pagineLaser Coaching: A Condensed 360 Coaching Experience To Increase Your Leaders' Confidence and ImpactPrune NivabeNessuna valutazione finora
- Rup VolvoDocumento22 pagineRup Volvoisabelita55100% (1)
- Critique Paper No.2 Rizal in The Context of 19th Century PhilippinesDocumento3 pagineCritique Paper No.2 Rizal in The Context of 19th Century PhilippinesMalia PolintanNessuna valutazione finora
- Scholarship Application Form: TBS - Scholarships@tcd - IeDocumento2 pagineScholarship Application Form: TBS - Scholarships@tcd - IeRoney GeorgeNessuna valutazione finora
- MAMBRASAR, S.PDDocumento2 pagineMAMBRASAR, S.PDAis MNessuna valutazione finora
- REVIEW of Reza Zia-Ebrahimi's "The Emergence of Iranian Nationalism: Race and The Politics of Dislocation"Documento5 pagineREVIEW of Reza Zia-Ebrahimi's "The Emergence of Iranian Nationalism: Race and The Politics of Dislocation"Wahid AzalNessuna valutazione finora
- Little Science Big Science and BeyondDocumento336 pagineLittle Science Big Science and Beyondadmin100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Gonzalez SanmamedDocumento14 pagineGonzalez SanmamedGuadalupe TenagliaNessuna valutazione finora
- Parenting Style Assessment PDFDocumento4 pagineParenting Style Assessment PDFAbyssman ManNessuna valutazione finora
- Vasquez, Jay Lord U.: PRK 3, Brgy. Guinacutan, Vinzons, Camarines Norte Mobile No.:09076971555Documento4 pagineVasquez, Jay Lord U.: PRK 3, Brgy. Guinacutan, Vinzons, Camarines Norte Mobile No.:09076971555choloNessuna valutazione finora
- Jennifer Valencia Disciplinary Literacy PaperDocumento8 pagineJennifer Valencia Disciplinary Literacy Paperapi-487420741Nessuna valutazione finora
- Knowledge: Skills: Attitude: ValuesDocumento3 pagineKnowledge: Skills: Attitude: ValuesVincent Paul TepaitNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)