Potrebbero piacerti anche
- Spinal Cord Deseases: Na ShaoDocumento38 pagineSpinal Cord Deseases: Na ShaoArvindhanNessuna valutazione finora
- Differentials and Tests Condition Condition: TH THDocumento4 pagineDifferentials and Tests Condition Condition: TH THlawlor_jcNessuna valutazione finora
- Xiao Luohan Quan 老架罗汉拳Documento25 pagineXiao Luohan Quan 老架罗汉拳Shaolin MeditatorNessuna valutazione finora
- Substance Abuse and Traumatic Brain Injury: John D. Corrigan, PHDDocumento50 pagineSubstance Abuse and Traumatic Brain Injury: John D. Corrigan, PHDSilvanaPutriNessuna valutazione finora
- Understanding the Motor and Sensory SystemsDocumento27 pagineUnderstanding the Motor and Sensory SystemschawkatNessuna valutazione finora
- Low Back Pain Differential DiagnosisDocumento58 pagineLow Back Pain Differential DiagnosisLusi UtamiNessuna valutazione finora
- Motor Imagery and MirrorTherapyDocumento5 pagineMotor Imagery and MirrorTherapyLorenaMariaNessuna valutazione finora
- A Simple Guide to Pick Disease, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Pick Disease, Diagnosis, Treatment and Related ConditionsValutazione: 5 su 5 stelle5/5 (1)
- 6 Minute Walk Test Vs Shuttle Walk TestDocumento3 pagine6 Minute Walk Test Vs Shuttle Walk TestcpradheepNessuna valutazione finora
- Headache: Prepared byDocumento23 pagineHeadache: Prepared byjawad_ahmedNessuna valutazione finora
- Pathophysiology of Traumatic Brain Injury: Kirsty J. DixonDocumento11 paginePathophysiology of Traumatic Brain Injury: Kirsty J. DixonalyaNessuna valutazione finora
- Cardiac Rehabilitation ArchitectureDocumento43 pagineCardiac Rehabilitation ArchitectureLevy McGardenNessuna valutazione finora
- Seizure Disorder, Spinal Injury Neural TumorDocumento52 pagineSeizure Disorder, Spinal Injury Neural TumornipoNessuna valutazione finora
- Peripheral Nerve DisordersDocumento34 paginePeripheral Nerve DisordersEddie WyattNessuna valutazione finora
- Surgical Incisions of Lower LimbDocumento11 pagineSurgical Incisions of Lower LimbcpradheepNessuna valutazione finora
- Balance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementDa EverandBalance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementNessuna valutazione finora
- 2012-04-24 FK PainDocumento49 pagine2012-04-24 FK PainYanis Widhiya NingrumNessuna valutazione finora
- Body Systems (Grade 6) - Free Printable Tests and Worksheets - HelpTeachingDocumento1 paginaBody Systems (Grade 6) - Free Printable Tests and Worksheets - HelpTeachingshuganesh82% (11)
- Traumatic Brain Injury: Shantaveer Gangu Mentor-Dr - Baldauf MDDocumento53 pagineTraumatic Brain Injury: Shantaveer Gangu Mentor-Dr - Baldauf MDRio AlexanderNessuna valutazione finora
- Cawthorne Cooksey Vertigo ExercisesDocumento1 paginaCawthorne Cooksey Vertigo Exercisescpradheep100% (1)
- Ortho Conus Medullaris and Cauda Equina SyndromeDocumento16 pagineOrtho Conus Medullaris and Cauda Equina Syndromemohamed100% (1)
- 6 Minute Walk Test ATS GuidelinesDocumento7 pagine6 Minute Walk Test ATS GuidelinescpradheepNessuna valutazione finora
- Spinal Cord Injury: Causation & PathophysiologyDocumento10 pagineSpinal Cord Injury: Causation & Pathophysiologycpradheep100% (3)
- Traumatic Brain Injury (TBI) - Definition, Epidemiology, PathophysiologyDocumento10 pagineTraumatic Brain Injury (TBI) - Definition, Epidemiology, Pathophysiologypetremure2147Nessuna valutazione finora
- Endocrine SystemDocumento21 pagineEndocrine SystemNo Name100% (1)
- Acute Spinal Cord InjuryDocumento3 pagineAcute Spinal Cord InjuryMarisol Dellera ValmoriaNessuna valutazione finora
- Blood Pressure and The Brain The Neurology of Hypertension PDFDocumento12 pagineBlood Pressure and The Brain The Neurology of Hypertension PDFGustavo PestanaNessuna valutazione finora
- Vestibular Neutitis & Labyrinthitis PDFDocumento6 pagineVestibular Neutitis & Labyrinthitis PDFFika Khulma SofiaNessuna valutazione finora
- Cast and TractionsDocumento3 pagineCast and TractionsMacaRonie PepeRownie del RioNessuna valutazione finora
- Emergency Clinical Diagnosis 2017Documento292 pagineEmergency Clinical Diagnosis 2017Ouma KinéNessuna valutazione finora
- Ultrasound Guided Lower Limb Blocks Tony AllenDocumento39 pagineUltrasound Guided Lower Limb Blocks Tony Allenrepre64Nessuna valutazione finora
- Unified Parkinson's Disease Rating Scale (UPDRS)Documento5 pagineUnified Parkinson's Disease Rating Scale (UPDRS)cpradheepNessuna valutazione finora
- Nerve Injury of Upper LimbDocumento41 pagineNerve Injury of Upper LimbbashirjnmcNessuna valutazione finora
- Spinal Cord Injury Assessment Chart (ASIA)Documento2 pagineSpinal Cord Injury Assessment Chart (ASIA)cpradheep100% (5)
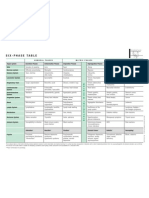
- Six-Phase Table: International Society of HomotoxicologyDocumento1 paginaSix-Phase Table: International Society of HomotoxicologyPablo Matas SoriaNessuna valutazione finora
- Acute AgitationDocumento83 pagineAcute AgitationSamuel FikaduNessuna valutazione finora
- Stroke Rsu Banjar: DR Fuad Hanif Sps M.KesDocumento80 pagineStroke Rsu Banjar: DR Fuad Hanif Sps M.KesRobert HarrisNessuna valutazione finora
- ANCA Associated VasculitisDocumento62 pagineANCA Associated VasculitispoluashokNessuna valutazione finora
- Zygomatic FractureDocumento13 pagineZygomatic FractureHippocrates Impressionist CostalesNessuna valutazione finora
- The Parkinson's Effect: R&R (Recommendations and Reasons)Da EverandThe Parkinson's Effect: R&R (Recommendations and Reasons)Nessuna valutazione finora
- N C C N D: Ursing ARE OF Lients With Eurologic IsordersDocumento96 pagineN C C N D: Ursing ARE OF Lients With Eurologic IsordersMatt Lao DionelaNessuna valutazione finora
- ICD 9 (Tindakan)Documento5 pagineICD 9 (Tindakan)supervisor rsualfatahNessuna valutazione finora
- Nuero RehabilitationDocumento127 pagineNuero RehabilitationPrajeesh ValayamkunnathNessuna valutazione finora
- Multiple MS Is Lyme Neuro BorrelioseDocumento8 pagineMultiple MS Is Lyme Neuro BorrelioseТатяна ТодороваNessuna valutazione finora
- Head InjuryDocumento31 pagineHead InjuryBoby SuryawanNessuna valutazione finora
- The Endocrine Systems How The Body WorksDocumento3 pagineThe Endocrine Systems How The Body Worksapi-441462208Nessuna valutazione finora
- Neurological Manifestations of Vascular DementiaDocumento5 pagineNeurological Manifestations of Vascular DementiaDumitruAuraNessuna valutazione finora
- Spina Bifida OCCULTADocumento1 paginaSpina Bifida OCCULTArebelswanteddot_comNessuna valutazione finora
- Conus Medullaris Vs Cauda Equina SyndromeDocumento1 paginaConus Medullaris Vs Cauda Equina SyndromecpradheepNessuna valutazione finora
- CINAHL Review StrokeDocumento9 pagineCINAHL Review Stroke28111966Nessuna valutazione finora
- Cauda Equina and Conus Medullaris Syndromes Clinical PresentationDocumento9 pagineCauda Equina and Conus Medullaris Syndromes Clinical PresentationhoneyworksNessuna valutazione finora
- Conus Medullaris and Cauda Equina SyndromesDocumento18 pagineConus Medullaris and Cauda Equina SyndromesAt Tha PholNessuna valutazione finora
- Stroke RehabDocumento20 pagineStroke Rehabapi-214830806Nessuna valutazione finora
- Compiled Stroke RehabDocumento121 pagineCompiled Stroke RehabJeel MohtaNessuna valutazione finora
- Rehab - NotesDocumento8 pagineRehab - Noteschris blacNessuna valutazione finora
- Cerebellar Stroke Causes, Symptoms & TreatmentDocumento17 pagineCerebellar Stroke Causes, Symptoms & TreatmentAna CotomanNessuna valutazione finora
- Causes of Weakness of Lower Limbs by DR Bashir Ahmed Dar Chinkipora Sopore KashmirDocumento23 pagineCauses of Weakness of Lower Limbs by DR Bashir Ahmed Dar Chinkipora Sopore KashmirProf Dr Bashir Ahmed Dar Chinki Pora Sopore Kashmir100% (1)
- MF2 - Spinal Cord InjuryDocumento43 pagineMF2 - Spinal Cord InjuryAnnbe BarteNessuna valutazione finora
- Gait Analysis GuideDocumento4 pagineGait Analysis GuideMokibul100% (1)
- Central Sensitisation Another Label or Useful DiagnosisDocumento4 pagineCentral Sensitisation Another Label or Useful DiagnosisMohamed ElMeligieNessuna valutazione finora
- Cauda Vs ConusDocumento7 pagineCauda Vs ConusDaniel Alon100% (2)
- Care Plan Exercise: Cristi Day RN, MSN, FNP-C Texas A&M University - Corpus ChristiDocumento19 pagineCare Plan Exercise: Cristi Day RN, MSN, FNP-C Texas A&M University - Corpus ChristiPhyu Lin0% (1)
- Sequelae of Trumatic Brain InjuryDocumento19 pagineSequelae of Trumatic Brain InjuryAnurag SuryawanshiNessuna valutazione finora
- Seminar On Gait Rehab in PDDocumento41 pagineSeminar On Gait Rehab in PDPriya KuberanNessuna valutazione finora
- Pathophysiology and Treatment of Tinnitus: An Elusive DiseaseDocumento11 paginePathophysiology and Treatment of Tinnitus: An Elusive DiseaseLyvie HarianiNessuna valutazione finora
- Health QuestionaireDocumento4 pagineHealth Questionaireapi-269450405Nessuna valutazione finora
- Seizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityDocumento50 pagineSeizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityArvindhanNessuna valutazione finora
- Quadrilatral and Ischial SocketDocumento133 pagineQuadrilatral and Ischial Socketjay prakashNessuna valutazione finora
- Bladder and Bowel Dysfunction in SCI Patients: Management StrategiesDocumento45 pagineBladder and Bowel Dysfunction in SCI Patients: Management StrategiesAbbas JafarzadehabbasNessuna valutazione finora
- Diabetic Peripheral NeuropathyDocumento13 pagineDiabetic Peripheral NeuropathygianisaNessuna valutazione finora
- Foot DropDocumento64 pagineFoot DropRam Chandra Reddy100% (1)
- ACUTE CONFUSIONAL STATE KoreksiDocumento39 pagineACUTE CONFUSIONAL STATE KoreksiMuhammad Afief100% (1)
- Parkinson's DiseaseDocumento3 pagineParkinson's Diseasehady920Nessuna valutazione finora
- 6 - Lumbar Disc HerniationDocumento24 pagine6 - Lumbar Disc HerniationHADI BADWANNessuna valutazione finora
- Brainstem Lesions GuideDocumento107 pagineBrainstem Lesions GuideAndrei ChyzhNessuna valutazione finora
- Facet Joint SyndromeDocumento17 pagineFacet Joint Syndromepaulvaso27100% (1)
- Kidney in Blood Pressure RegulationDocumento22 pagineKidney in Blood Pressure RegulationcpradheepNessuna valutazione finora
- Clinical Manifestation of Acute Spinal Cord Injury, Chapter-4Documento6 pagineClinical Manifestation of Acute Spinal Cord Injury, Chapter-4cpradheepNessuna valutazione finora
- Spinal Cord Injury Bladder Management-1Documento3 pagineSpinal Cord Injury Bladder Management-1cpradheepNessuna valutazione finora
- Spinal Cord Injury Bladder Management-2Documento3 pagineSpinal Cord Injury Bladder Management-2cpradheepNessuna valutazione finora
- Spinal Cord BasicsDocumento2 pagineSpinal Cord BasicscpradheepNessuna valutazione finora
- Conversion Disorder: Background: Conversion Disorder Is Included As A Somatoform DisorderDocumento10 pagineConversion Disorder: Background: Conversion Disorder Is Included As A Somatoform Disordercpradheep0% (1)
- Understanding Girdle Stone ProcedureDocumento8 pagineUnderstanding Girdle Stone ProcedurecpradheepNessuna valutazione finora
- What Is Critical AppraisalDocumento8 pagineWhat Is Critical AppraisalcpradheepNessuna valutazione finora
- Hip Fracture Management New Zealand Best Practice GuidelinesDocumento40 pagineHip Fracture Management New Zealand Best Practice GuidelinescpradheepNessuna valutazione finora
- Falls Prevention Gait Tips For ElderlyDocumento2 pagineFalls Prevention Gait Tips For ElderlycpradheepNessuna valutazione finora
- Etiopathology & Treatment Related Aspects of Hip FractureDocumento75 pagineEtiopathology & Treatment Related Aspects of Hip FracturecpradheepNessuna valutazione finora
- Baxi 80HE Combi Heater - User's Operating InstructionsDocumento12 pagineBaxi 80HE Combi Heater - User's Operating InstructionscpradheepNessuna valutazione finora
- Falls Prevention Gait Tips For ElderlyDocumento2 pagineFalls Prevention Gait Tips For ElderlycpradheepNessuna valutazione finora
- Outcome Measures Used in PVD / PADDocumento6 pagineOutcome Measures Used in PVD / PADcpradheep100% (2)
- Pakinson's Disease Fitness CountsDocumento48 paginePakinson's Disease Fitness CountscpradheepNessuna valutazione finora
- Parkinson's Disease ADL TipsDocumento48 pagineParkinson's Disease ADL Tipscpradheep100% (1)
- Fracture Spine CT Vs Xray Which Is BestDocumento8 pagineFracture Spine CT Vs Xray Which Is BestcpradheepNessuna valutazione finora
- Disability of The Arm, Shoulder and Hand (DASH)Documento4 pagineDisability of The Arm, Shoulder and Hand (DASH)cpradheepNessuna valutazione finora
- Falls Prevention - Safe FootwearDocumento1 paginaFalls Prevention - Safe FootwearcpradheepNessuna valutazione finora
- Prescribing Exercises For Frail EldersDocumento11 paginePrescribing Exercises For Frail ElderscpradheepNessuna valutazione finora
- Care Giver Stress IndexDocumento2 pagineCare Giver Stress IndexcpradheepNessuna valutazione finora
- Cauda Equina SyndromeDocumento3 pagineCauda Equina SyndromepuchioNessuna valutazione finora
- In The Name of Allah The Most Gracious The Most MercifulDocumento118 pagineIn The Name of Allah The Most Gracious The Most Mercifulkhlid21mtz100% (2)
- Stiff-Legged Deadlift Squat Thrust Weighted Pushup Weighted Pull-Ups Weighted DipsDocumento3 pagineStiff-Legged Deadlift Squat Thrust Weighted Pushup Weighted Pull-Ups Weighted DipsAJ ChoiNessuna valutazione finora
- 2014 Mrcs Osce RECALLDocumento85 pagine2014 Mrcs Osce RECALLIdo EgaziNessuna valutazione finora
- Kids Training ProgramDocumento1 paginaKids Training ProgramBruce KalbNessuna valutazione finora
- Close Combat Techniques (CCT)Documento15 pagineClose Combat Techniques (CCT)Rafael Samir GomezNessuna valutazione finora
- Types of MusclesDocumento23 pagineTypes of MusclesSONGA AmriNessuna valutazione finora
- Cardiac PacemakersDocumento3 pagineCardiac PacemakersDhruv SridharNessuna valutazione finora
- Unit 4 (Checked) - MMDocumento8 pagineUnit 4 (Checked) - MMkirana larastriNessuna valutazione finora
- Quantec Aamd PDFDocumento41 pagineQuantec Aamd PDFNika TopuriaNessuna valutazione finora
- Positions at a GlanceDocumento18 paginePositions at a GlanceRaquel M. MendozaNessuna valutazione finora
- Company - City Pincode Locality Sub - Localiaddress Building - Landmarksstdcode TelephoneDocumento3 pagineCompany - City Pincode Locality Sub - Localiaddress Building - Landmarksstdcode Telephonedeva nesanNessuna valutazione finora
- SMTHDocumento13 pagineSMTHblackghost-girlNessuna valutazione finora
- Anthropometry: 4.0 Scope of Anthropometry in Movement BiomechanicsDocumento25 pagineAnthropometry: 4.0 Scope of Anthropometry in Movement BiomechanicsJoel PPPNessuna valutazione finora
- Fe Neko or Dog or CatDocumento30 pagineFe Neko or Dog or CatSomething PowerfulNessuna valutazione finora
- Hemodynamics The Study of The Movement of Blood and The Physical Principles Governing This MovementDocumento46 pagineHemodynamics The Study of The Movement of Blood and The Physical Principles Governing This MovementwayneNessuna valutazione finora
- Volkmann Contracture Causes, Symptoms, and TreatmentDocumento4 pagineVolkmann Contracture Causes, Symptoms, and TreatmentAdre RefdianNessuna valutazione finora
- Section - 035 - Denture Occlusion OverviewDocumento3 pagineSection - 035 - Denture Occlusion OverviewAravind KrishnanNessuna valutazione finora
- Conduction System of The HeartDocumento1 paginaConduction System of The HeartJulie AnnNessuna valutazione finora
- Review of The Autonomic Nervous SystemDocumento31 pagineReview of The Autonomic Nervous SystemBelleNessuna valutazione finora
- SC f3 (KSSM) Notes 1.2Documento13 pagineSC f3 (KSSM) Notes 1.2Kah Yee LaiNessuna valutazione finora