Potrebbero piacerti anche
- Surgery: by DR - Mohammad Z. Abu Sheikha@Documento145 pagineSurgery: by DR - Mohammad Z. Abu Sheikha@صقر حورانNessuna valutazione finora
- Step 1 UW Objectives Subjectwise 2022Documento474 pagineStep 1 UW Objectives Subjectwise 2022saranya sankarNessuna valutazione finora
- Mo Intern Handbook - FinalDocumento37 pagineMo Intern Handbook - FinalGideon K. MutaiNessuna valutazione finora
- Rapid Infusion for Hypovolemic ShockDocumento11 pagineRapid Infusion for Hypovolemic ShocksasghfdgNessuna valutazione finora
- Paediatrics & Biostatistics Notes - USMLE Step 2CKDocumento102 paginePaediatrics & Biostatistics Notes - USMLE Step 2CKDuncan89Nessuna valutazione finora
- 100 Commonly Tested Facts For MRCP Part 1Documento5 pagine100 Commonly Tested Facts For MRCP Part 1Khalid AbdelazizNessuna valutazione finora
- U.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3Documento5 pagineU.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3mtataNessuna valutazione finora
- Emma Holliday Surgery Notes - Cornell StyleDocumento299 pagineEmma Holliday Surgery Notes - Cornell StyleBanana MuffinNessuna valutazione finora
- Third-Year OSCE Manual 2019-2020Documento17 pagineThird-Year OSCE Manual 2019-2020Agleema AhmedNessuna valutazione finora
- USMLE Step 2 CK 6 Months Study Plan For 240Documento1 paginaUSMLE Step 2 CK 6 Months Study Plan For 240DhritisdiaryNessuna valutazione finora
- Assessment of the Politraumatized PatientDa EverandAssessment of the Politraumatized PatientNessuna valutazione finora
- Main Dip Step 2ck Notes Info Doc - Read OnlyDocumento305 pagineMain Dip Step 2ck Notes Info Doc - Read Only[161]Shuaib AktherNessuna valutazione finora
- General Surgery Study GuideDocumento118 pagineGeneral Surgery Study GuideYvonne HuangNessuna valutazione finora
- High Yield Step 2ckDocumento4 pagineHigh Yield Step 2ckCesar_Palana_3832Nessuna valutazione finora
- Uworld BiostatisticsDocumento2 pagineUworld BiostatisticsКостянтин РоманівNessuna valutazione finora
- Orientation To General SurgeryDocumento0 pagineOrientation To General SurgeryIrham TahkikNessuna valutazione finora
- SoCal's UW Step 2 CK EOs (UTD 10 Nov)Documento292 pagineSoCal's UW Step 2 CK EOs (UTD 10 Nov)JJ0% (1)
- US Navy Course NAVEDTRA 14274 - Dental Technician Vol 1Documento290 pagineUS Navy Course NAVEDTRA 14274 - Dental Technician Vol 1Georges100% (3)
- Abrupta Placenta - 4 Pt presents with vaginal bleeding, ABDOMINAL PAIN, and uterine tendernessDocumento211 pagineAbrupta Placenta - 4 Pt presents with vaginal bleeding, ABDOMINAL PAIN, and uterine tendernessroad2successNessuna valutazione finora
- Amboss Hemolytic AnemiaDocumento16 pagineAmboss Hemolytic AnemiaAhmed Ali100% (2)
- Medical Ethics NotesDocumento11 pagineMedical Ethics NotesMuhammad Waqar RehanNessuna valutazione finora
- Risk Factors - Step 2 PDFDocumento5 pagineRisk Factors - Step 2 PDFAmberNessuna valutazione finora
- YFT IM Notes 1Documento100 pagineYFT IM Notes 1AHMAD ALROWAILYNessuna valutazione finora
- Aquifer Case - Summary - FamilyMedicine21 - 12-YDocumento10 pagineAquifer Case - Summary - FamilyMedicine21 - 12-YHyunsoo EllisNessuna valutazione finora
- Infants and ToddlersDocumento14 pagineInfants and ToddlersJosias Smith100% (1)
- Stroke RecoveryDocumento20 pagineStroke RecoveryVanessa SnowNessuna valutazione finora
- 803 Service ManualDocumento196 pagine803 Service Manualвася рогов100% (1)
- Aquifer Case - Summary - FamilyMedicine23 - 5-YeDocumento9 pagineAquifer Case - Summary - FamilyMedicine23 - 5-YeHyunsoo EllisNessuna valutazione finora
- Epi Cheatsheet PDFDocumento4 pagineEpi Cheatsheet PDFDrbee10Nessuna valutazione finora
- Smhs - Gwu.edu Sample NotesDocumento3 pagineSmhs - Gwu.edu Sample NotesWaqas HaleemNessuna valutazione finora
- Care Plan Handbook TemplateDocumento34 pagineCare Plan Handbook TemplateBreanna Hopkins100% (1)
- Oral Case Presentation Benchmarks - : Identifying Information & Chief ConcernDocumento9 pagineOral Case Presentation Benchmarks - : Identifying Information & Chief ConcernManisanthosh KumarNessuna valutazione finora
- Uw Step 2 CK Im H ODocumento67 pagineUw Step 2 CK Im H OAilyn MNessuna valutazione finora
- ICU Presentation - Systems BasedDocumento1 paginaICU Presentation - Systems BasedBryan NomenNessuna valutazione finora
- Guide To The OBGYN Shelf - StepwardsDocumento5 pagineGuide To The OBGYN Shelf - StepwardsJamesHowsonNessuna valutazione finora
- UVA Family QuestionsDocumento30 pagineUVA Family QuestionsSamuel RothschildNessuna valutazione finora
- Clinical Examinations Crib Sheet v7Documento36 pagineClinical Examinations Crib Sheet v7aparish10100% (1)
- Peds Shelf NotesDocumento88 paginePeds Shelf Notesγιαννης παπαςNessuna valutazione finora
- USMLE HY Internal Medicine Random FactoidsDocumento18 pagineUSMLE HY Internal Medicine Random FactoidsHugo SalinasNessuna valutazione finora
- 7-Week Usmle Step 1 Sample ScheduleDocumento2 pagine7-Week Usmle Step 1 Sample ScheduleHannah ChanNessuna valutazione finora
- How To Study For Third Year Rotations PDFDocumento5 pagineHow To Study For Third Year Rotations PDFAudia IndrianNessuna valutazione finora
- Obesteric Gynacology Short Notes For Usmle Step 2Documento32 pagineObesteric Gynacology Short Notes For Usmle Step 2Rodaba Ahmadi Meherzad100% (1)
- Gynecology and ObstetricsvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvDocumento133 pagineGynecology and ObstetricsvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvȚurcan IurieNessuna valutazione finora
- UntitledDocumento193 pagineUntitledurosNessuna valutazione finora
- Msec m3 Guide 2018 PDFDocumento101 pagineMsec m3 Guide 2018 PDFSibel GafarNessuna valutazione finora
- ASTM D1123 Contenido Agua en Glicol PDFDocumento5 pagineASTM D1123 Contenido Agua en Glicol PDFdianacalixtogNessuna valutazione finora
- Process Description of Gambat South Gas Processing FacilityDocumento13 pagineProcess Description of Gambat South Gas Processing FacilitywaheedNessuna valutazione finora
- Hoja de Seguridad Magnafloc 155 (EN) PDFDocumento6 pagineHoja de Seguridad Magnafloc 155 (EN) PDFIván Martínez-CostaNessuna valutazione finora
- HY Mixed USMLE Review Part I 1Documento20 pagineHY Mixed USMLE Review Part I 1Jennifer Ross-ComptisNessuna valutazione finora
- Konseling Kreatif Dan Jarak JauhDocumento66 pagineKonseling Kreatif Dan Jarak JauhNindyani BudiNessuna valutazione finora
- Boge Screw UsaDocumento40 pagineBoge Screw UsaAir Repair, LLC100% (1)
- Ukite 2011Documento123 pagineUkite 2011pikacu19650% (2)
- Wu Step 2 CK Study PlanDocumento5 pagineWu Step 2 CK Study PlanLeti Sefa TaNessuna valutazione finora
- The Yale Way - New Patient PresentationsDocumento9 pagineThe Yale Way - New Patient PresentationsAndrew McGowanNessuna valutazione finora
- The AOA Guide:: How To Succeed in The Third-Year ClerkshipsDocumento25 pagineThe AOA Guide:: How To Succeed in The Third-Year Clerkshipshector100% (1)
- IBC CODE - International Code For The Construction and Equipment of Ships CarryiDocumento9 pagineIBC CODE - International Code For The Construction and Equipment of Ships CarryiLuka KriletićNessuna valutazione finora
- Deconstructing The ECG Curve - The Components of The Tracing: Key ConceptsDocumento117 pagineDeconstructing The ECG Curve - The Components of The Tracing: Key ConceptsdrynwhylNessuna valutazione finora
- DeVirglio NotesDocumento77 pagineDeVirglio NotesAlvand SehatNessuna valutazione finora
- Shoulder dystocia management and PPH treatmentDocumento9 pagineShoulder dystocia management and PPH treatmentJeffrey HingNessuna valutazione finora
- SOAP Presentation 5.19.16 PDFDocumento1 paginaSOAP Presentation 5.19.16 PDFnems92Nessuna valutazione finora
- Gynecology StudyguideDocumento39 pagineGynecology StudyguideGameron777Nessuna valutazione finora
- Family Medicine PresentationDocumento53 pagineFamily Medicine PresentationNancy BaggaNessuna valutazione finora
- Sunday: (Flashcards) (Flashcards) (Flashcards)Documento10 pagineSunday: (Flashcards) (Flashcards) (Flashcards)Miruu NaNessuna valutazione finora
- Aquifer InternalMedicine09 - 55Documento7 pagineAquifer InternalMedicine09 - 55JulieNessuna valutazione finora
- Aquifer InternalMedicine11 - 45Documento8 pagineAquifer InternalMedicine11 - 45JulieNessuna valutazione finora
- SketchyPath ChecklistDocumento1 paginaSketchyPath ChecklistFajar Raza100% (1)
- Obstetrics and Gynecology Clerkship OverviewDocumento16 pagineObstetrics and Gynecology Clerkship Overviewselvie8750% (2)
- USMLE Step 2 CS Patient Interview TemplateDocumento2 pagineUSMLE Step 2 CS Patient Interview Templatet0raken75% (4)
- Divine Intervention Episode 69 Usmle Anatomy Series Part 2Documento9 pagineDivine Intervention Episode 69 Usmle Anatomy Series Part 2Swisskelly1Nessuna valutazione finora
- Medical TourismDocumento18 pagineMedical TourismdhnaushNessuna valutazione finora
- Proforma For Iphs Facility Survey of SCDocumento6 pagineProforma For Iphs Facility Survey of SCSandip PatilNessuna valutazione finora
- Asrs For AutomationDocumento25 pagineAsrs For AutomationJavedNessuna valutazione finora
- XFY1548移动式筛分站术规格书Documento16 pagineXFY1548移动式筛分站术规格书abangNessuna valutazione finora
- Chem For Engineering Material by Pup BuddiesDocumento46 pagineChem For Engineering Material by Pup BuddiesJedidiah MondaresNessuna valutazione finora
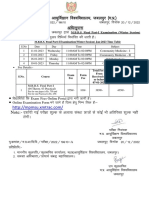
- MBBS Final Part-I (Winter Session) Time Table (Jan 2023)Documento1 paginaMBBS Final Part-I (Winter Session) Time Table (Jan 2023)crystal mindNessuna valutazione finora
- Report On Baby Food Industry in BangladeshDocumento5 pagineReport On Baby Food Industry in BangladeshIffatur RahmanNessuna valutazione finora
- The Baking and Frozen Dough MarketDocumento4 pagineThe Baking and Frozen Dough MarketMilling and Grain magazineNessuna valutazione finora
- Councillor Danny Thorpe: Leader, Royal Borough of GreenwichDocumento2 pagineCouncillor Danny Thorpe: Leader, Royal Borough of GreenwichDr-Syed Ali TarekNessuna valutazione finora
- Adapted Sports & Recreation 2015: The FCPS Parent Resource CenterDocumento31 pagineAdapted Sports & Recreation 2015: The FCPS Parent Resource CenterkirthanasriNessuna valutazione finora
- Saloni Shah - LLM DissertationDocumento156 pagineSaloni Shah - LLM DissertationNilesh BatraNessuna valutazione finora
- A.686 (17) Cod AlarmeDocumento39 pagineA.686 (17) Cod Alarmeciocioi iancuNessuna valutazione finora
- Airtel's Africa Growth: Surviving CompetitionDocumento9 pagineAirtel's Africa Growth: Surviving CompetitionSagar RiazNessuna valutazione finora
- Nescafe Alegria Nutritional Facts PDFDocumento3 pagineNescafe Alegria Nutritional Facts PDFOmarNessuna valutazione finora
- Bemidji Police Department 1-14-13Documento19 pagineBemidji Police Department 1-14-13John HagemanNessuna valutazione finora
- Homes & Diamonds of Liz TaylorDocumento42 pagineHomes & Diamonds of Liz TaylorFridayFunStuffNessuna valutazione finora
- Causes & Prevention of Coronary Artery DiseaseDocumento41 pagineCauses & Prevention of Coronary Artery DiseaseeenagpurcongNessuna valutazione finora
- ImpetigoDocumento31 pagineImpetigoUmmu Insyirah100% (1)