Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Diff Betwn Inlay and Amalgam CavityDocumento7 pagineDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Criteria of SelectionDocumento12 pagineCriteria of SelectionVinisha Vipin SharmaNessuna valutazione finora
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocumento159 pagineMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaNessuna valutazione finora
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocumento6 pagineNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNessuna valutazione finora
- Acupuncture in Dentistry PDFDocumento73 pagineAcupuncture in Dentistry PDFVinisha Vipin SharmaNessuna valutazione finora
- Challenges in Working Length DeterminationDocumento101 pagineChallenges in Working Length DeterminationVinisha Vipin SharmaNessuna valutazione finora
- Eaat 14 I 1 P 217Documento6 pagineEaat 14 I 1 P 217Vinisha Vipin SharmaNessuna valutazione finora
- Content ServerDocumento5 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
- Glide Path PreparationDocumento5 pagineGlide Path PreparationVinisha Vipin SharmaNessuna valutazione finora
- Show TextDocumento1 paginaShow TextVinisha Vipin SharmaNessuna valutazione finora
- PRISMA-P Statement - Moher Sys Rev Jan 2015Documento9 paginePRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaNessuna valutazione finora
- Some Basics of LasersDocumento102 pagineSome Basics of LasersVinisha Vipin SharmaNessuna valutazione finora
- Laser in Conservative Dentistry & EndodonticsDocumento75 pagineLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaNessuna valutazione finora
- Dentin HypersensitivityDocumento62 pagineDentin HypersensitivityVinisha Vipin Sharma100% (1)
- Content ServerDocumento6 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
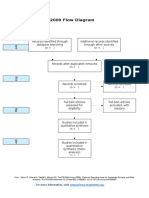
- PRISMA 2009 Flow Diagram: For More Information, VisitDocumento1 paginaPRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaNessuna valutazione finora
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDocumento5 paginePractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaNessuna valutazione finora
- EchsDocumento20 pagineEchsVinisha Vipin SharmaNessuna valutazione finora
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocumento5 pagineCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaNessuna valutazione finora
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocumento5 pagineNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaNessuna valutazione finora
- Esthetic Alternatives To AmalgamDocumento15 pagineEsthetic Alternatives To AmalgamVinisha Vipin SharmaNessuna valutazione finora
- Pin Retained RestorationDocumento31 paginePin Retained RestorationVinisha Vipin SharmaNessuna valutazione finora
- Clarks Cavity PreparationDocumento10 pagineClarks Cavity PreparationVinisha Vipin SharmaNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Warm Blooded Animals & ThermoregulationDocumento33 pagineWarm Blooded Animals & Thermoregulationlock stock and barrelNessuna valutazione finora
- Arterial Tortuosity SyndromeDocumento11 pagineArterial Tortuosity SyndromeNawal RaiNessuna valutazione finora
- IELTS Practice ReadingDocumento6 pagineIELTS Practice ReadingAhamed Areeb100% (1)
- Characterization of The Chemical Composition of Adenostemma Lavenia (L.) Kuntze and Adenostemma Platyphyllum CassDocumento9 pagineCharacterization of The Chemical Composition of Adenostemma Lavenia (L.) Kuntze and Adenostemma Platyphyllum Casszan_anwarNessuna valutazione finora
- Lesson Plan For Demo TeachingDocumento6 pagineLesson Plan For Demo Teachingjanice alquizar100% (6)
- Labmax 240Documento43 pagineLabmax 240Dharmesh PatelNessuna valutazione finora
- Diagnostic Test Science 10Documento8 pagineDiagnostic Test Science 10Pilar Angelie Palmares VillarinNessuna valutazione finora
- Erotic MassageDocumento2 pagineErotic MassageKarugu MartinNessuna valutazione finora
- FoshuDocumento11 pagineFoshuEducapec EcuadorNessuna valutazione finora
- % de Agu en PectinaDocumento89 pagine% de Agu en PectinaMayra Valdivieso100% (1)
- Review Session in Licensure Examination For Agriculturist (Lea)Documento168 pagineReview Session in Licensure Examination For Agriculturist (Lea)Phoebe O. TumammanNessuna valutazione finora
- RGKSU 1st Proff 10 YearsDocumento115 pagineRGKSU 1st Proff 10 YearsAranya BhandaryNessuna valutazione finora
- CPB 30103 Biochemical Engineering UniKL MICET Experiment 4: Determination of Bacterial Loads Viable Cell Counts Full Lab ReportDocumento12 pagineCPB 30103 Biochemical Engineering UniKL MICET Experiment 4: Determination of Bacterial Loads Viable Cell Counts Full Lab ReportSiti Hajar Mohamed100% (2)
- PVP Form 1-Application FormDocumento7 paginePVP Form 1-Application FormJoeluntalanNessuna valutazione finora
- History of HLA PDFDocumento17 pagineHistory of HLA PDFeseNessuna valutazione finora
- Spermatogenesis PPTDocumento42 pagineSpermatogenesis PPTInsatiable CleeNessuna valutazione finora
- Letter Hon. D. LeBlanc - Miramichi LakeDocumento15 pagineLetter Hon. D. LeBlanc - Miramichi LakeNeville CrabbeNessuna valutazione finora
- Extended BodyDocumento5 pagineExtended BodyHyphae ProjectNessuna valutazione finora
- Biomolecules - DPP 01 - (Pravesh 2.0)Documento4 pagineBiomolecules - DPP 01 - (Pravesh 2.0)kd79329Nessuna valutazione finora
- Identifying Human Versus Non-Human Skeletal Remains in The FieldDocumento24 pagineIdentifying Human Versus Non-Human Skeletal Remains in The FieldVasantha PhutaneNessuna valutazione finora
- Inter 1 Biology Success SeriesDocumento8 pagineInter 1 Biology Success Seriesashfaq4985Nessuna valutazione finora
- 1 s2.0 S1319562X19300968 MainDocumento11 pagine1 s2.0 S1319562X19300968 MainRobert TriarjunetNessuna valutazione finora
- Green Pesticides For Organic Farming Occurrence and Properties of Essential Oils For Use in Pest ControlDocumento25 pagineGreen Pesticides For Organic Farming Occurrence and Properties of Essential Oils For Use in Pest ControlteguhwidiartoNessuna valutazione finora
- Guide To Z Scores 1.2Documento9 pagineGuide To Z Scores 1.2Marco Vinicio Bazzotti100% (1)
- Hungarian Genetics, Madjars, Xiungnu, Tarim Basin, Huns, UyghurDocumento4 pagineHungarian Genetics, Madjars, Xiungnu, Tarim Basin, Huns, Uyghurfilippo_eneaNessuna valutazione finora
- Biological SciencesDocumento2 pagineBiological SciencesHNNessuna valutazione finora
- Crone Dahl 2012 NRNDocumento16 pagineCrone Dahl 2012 NRNFernandaNessuna valutazione finora
- Basics of Biomagnetism (Inglés) (Presentación) Autor Michael DungDocumento46 pagineBasics of Biomagnetism (Inglés) (Presentación) Autor Michael DungRodrigo BarraNessuna valutazione finora
- Dr. Diah Rumekti hadiatiAPCGS JogjaDocumento25 pagineDr. Diah Rumekti hadiatiAPCGS JogjacirererereNessuna valutazione finora
- Penicillium Rubens 774541 PDFDocumento153 paginePenicillium Rubens 774541 PDFParis LavinNessuna valutazione finora