
Potrebbero piacerti anche
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYDa EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNessuna valutazione finora
- Neurosurgery UpdateDocumento30 pagineNeurosurgery UpdateGustavo Xavier Ayarza PulidoNessuna valutazione finora
- Jo (2003)Documento5 pagineJo (2003)Елена КарпинскаяNessuna valutazione finora
- Altunoluk 2010Documento5 pagineAltunoluk 2010Merlin MuktialiNessuna valutazione finora
- JurnahDocumento6 pagineJurnahApriany Fitri SangajiNessuna valutazione finora
- Kumar S.Documento4 pagineKumar S.Van DaoNessuna valutazione finora
- Effect of Epidural Analgesia IDocumento14 pagineEffect of Epidural Analgesia IRhandy SeptiantoNessuna valutazione finora
- Bahan KedkelDocumento8 pagineBahan KedkelUliza Nur AiniNessuna valutazione finora
- Tens Po Toracolomia - SEZENDocumento5 pagineTens Po Toracolomia - SEZENKamylla Caroline SantosNessuna valutazione finora
- US For Epidural. Anesth Analg 2017Documento6 pagineUS For Epidural. Anesth Analg 2017tarekabdelkarem927Nessuna valutazione finora
- Sonnykalangi,+151 +Fiska+M+Muhammad+863-68Documento6 pagineSonnykalangi,+151 +Fiska+M+Muhammad+863-68Evieta CallysthaNessuna valutazione finora
- 1 s2.0 S1110184912001031 MainDocumento6 pagine1 s2.0 S1110184912001031 MainFenny KusumasariNessuna valutazione finora
- J Clin NeuroSc 14 - Time Interval To Surgery and Outcomes Following The Surgical Treatment of Actue Traumatic Subdural HematomaDocumento5 pagineJ Clin NeuroSc 14 - Time Interval To Surgery and Outcomes Following The Surgical Treatment of Actue Traumatic Subdural HematomaZeptAlanNessuna valutazione finora
- Alici 2001Documento2 pagineAlici 2001BudhiNessuna valutazione finora
- Bed Angels On PainDocumento12 pagineBed Angels On PainNiken AninditaNessuna valutazione finora
- Original Papers: Comparison of Shouldice and Lichtenstein Repair For Treatment of Primary Inguinal HerniaDocumento4 pagineOriginal Papers: Comparison of Shouldice and Lichtenstein Repair For Treatment of Primary Inguinal Herniahitesh315Nessuna valutazione finora
- Laparoscopic Vs Open Ventral Hernia RepairDocumento4 pagineLaparoscopic Vs Open Ventral Hernia RepairLouis FortunatoNessuna valutazione finora
- Articulo de HombroDocumento8 pagineArticulo de HombroYesenia OchoaNessuna valutazione finora
- The Effect of Surgical Timing On Operative Duration and Quality of Reduction in Type III Supracondylar Humeral Fractures in ChildrenDocumento6 pagineThe Effect of Surgical Timing On Operative Duration and Quality of Reduction in Type III Supracondylar Humeral Fractures in ChildrenshtefanazNessuna valutazione finora
- The Use of Theatre Time For Paed Dent Under GA FOLEY - Et - Al-2007Documento5 pagineThe Use of Theatre Time For Paed Dent Under GA FOLEY - Et - Al-2007NaseemNessuna valutazione finora
- Increasing Time To Operation Is Associated With Decreased Survival in Patients With A Positive FAST Examination Requiring Emergent LaparotomyDocumento5 pagineIncreasing Time To Operation Is Associated With Decreased Survival in Patients With A Positive FAST Examination Requiring Emergent LaparotomyEvelyn GrandaNessuna valutazione finora
- Post in GlycoDocumento4 paginePost in GlycoSA SHNessuna valutazione finora
- f194 DikonversiDocumento5 paginef194 DikonversiFarizka Dwinda HNessuna valutazione finora
- Return To Preinjury Status After Routine Knee Arthroscopy in Military PopulationDocumento5 pagineReturn To Preinjury Status After Routine Knee Arthroscopy in Military PopulationLuis MiguelNessuna valutazione finora
- Timing of Cranioplasty After Decompressive Craniectomy ForDocumento5 pagineTiming of Cranioplasty After Decompressive Craniectomy ForjoerizalNessuna valutazione finora
- Comparison of Pre Procedural and Real Time Ultrasound Guided Spinal Anesthesia For Traumatic Lower Limb InjuryDocumento7 pagineComparison of Pre Procedural and Real Time Ultrasound Guided Spinal Anesthesia For Traumatic Lower Limb InjuryIJAR JOURNALNessuna valutazione finora
- TKR 1Documento8 pagineTKR 1putriNessuna valutazione finora
- Tramadol en NiñosDocumento5 pagineTramadol en NiñosElias Vera RojasNessuna valutazione finora
- Timing of Surgery For Aneurysmal Subarachnoid Hemorrhage - A Systematic Review and Meta-AnalysisDocumento9 pagineTiming of Surgery For Aneurysmal Subarachnoid Hemorrhage - A Systematic Review and Meta-AnalysisJulieta PereyraNessuna valutazione finora
- Arroyo Novoa 2008Documento8 pagineArroyo Novoa 2008EviNessuna valutazione finora
- Br. J. Anaesth.-1994-LEITH-552-8Documento7 pagineBr. J. Anaesth.-1994-LEITH-552-8Anonymous V5l8nmcSxbNessuna valutazione finora
- Esp KPDocumento8 pagineEsp KPKrishna PrasadNessuna valutazione finora
- Research Article: Correlation Between TMD and Cervical Spine Pain and Mobility: Is The Whole Body Balance TMJ Related?Documento8 pagineResearch Article: Correlation Between TMD and Cervical Spine Pain and Mobility: Is The Whole Body Balance TMJ Related?gloriagaskNessuna valutazione finora
- 1 s2.0 S0883944116302167 MainDocumento5 pagine1 s2.0 S0883944116302167 MainEmilian EmNessuna valutazione finora
- 12Hiệu quả mở kq sớm pt gộp 2015Documento10 pagine12Hiệu quả mở kq sớm pt gộp 2015Cường Nguyễn HùngNessuna valutazione finora
- Anesth Analg 2009 Lee 252 4Documento3 pagineAnesth Analg 2009 Lee 252 4Ican DoitNessuna valutazione finora
- Impact of Time From Completion of Neoadjuvant Chemotherapy To Surgery On Survival Outcomes in Breast Cancer PatientsDocumento7 pagineImpact of Time From Completion of Neoadjuvant Chemotherapy To Surgery On Survival Outcomes in Breast Cancer PatientsPani lookyeeNessuna valutazione finora
- Safety of Robotic Thyroidectomy Approaches: Meta-Analysis and Systematic ReviewDocumento7 pagineSafety of Robotic Thyroidectomy Approaches: Meta-Analysis and Systematic Reviewcabeza y cuello incNessuna valutazione finora
- Standing With Assistance of A Tilt Table in Intensive Care: A Survey of Australian Physiotherapy PracticeDocumento4 pagineStanding With Assistance of A Tilt Table in Intensive Care: A Survey of Australian Physiotherapy PracticeXime JaneiroNessuna valutazione finora
- Impact of Time To Surgery After Neoadjuvant Chemotherapy in Operable Breast Cancer PatientsDocumento6 pagineImpact of Time To Surgery After Neoadjuvant Chemotherapy in Operable Breast Cancer PatientsPani lookyeeNessuna valutazione finora
- 1 s2.0 S0022480417303529 MainDocumento6 pagine1 s2.0 S0022480417303529 MainEva ArdianahNessuna valutazione finora
- Long-Term Outcomes of Immediate Repair Compared With Surveillance of Small Abdominal Aortic AneurysmsDocumento8 pagineLong-Term Outcomes of Immediate Repair Compared With Surveillance of Small Abdominal Aortic AneurysmsJason BiggyNessuna valutazione finora
- 2 DiaphragmaticExcursionDocumento4 pagine2 DiaphragmaticExcursionAnandhu GNessuna valutazione finora
- Transversus Abdominis Plane Block For Laparoscopic Inguinal Hernia Repair: A Randomized TrialDocumento8 pagineTransversus Abdominis Plane Block For Laparoscopic Inguinal Hernia Repair: A Randomized TrialAYŞE GÜLŞAH ATASEVERNessuna valutazione finora
- Sutureless Tympanoplasty Using Acellular DermisDocumento4 pagineSutureless Tympanoplasty Using Acellular DermissreshtamukhiNessuna valutazione finora
- Jurnal IbsDocumento6 pagineJurnal IbsRamaNessuna valutazione finora
- The Effects of Continuous and Interrupted Episiotomy Repair On Pain Severity and Rate of Perineal Repair: A Controlled Randomized Clinical TrialDocumento13 pagineThe Effects of Continuous and Interrupted Episiotomy Repair On Pain Severity and Rate of Perineal Repair: A Controlled Randomized Clinical TrialMarfuahRobertoNessuna valutazione finora
- Jurnal EswtDocumento13 pagineJurnal EswtnisahudaNessuna valutazione finora
- Vertebrplasty 2016Documento10 pagineVertebrplasty 2016karenNessuna valutazione finora
- Shannon - YFT - EVD - Editors - Comments (Second Round)Documento19 pagineShannon - YFT - EVD - Editors - Comments (Second Round)rabia khalidNessuna valutazione finora
- International Journal of Health Sciences and ResearchDocumento6 pagineInternational Journal of Health Sciences and Researchmekar retnoningsihNessuna valutazione finora
- Anesth Essays ResDocumento8 pagineAnesth Essays ResFi NoNessuna valutazione finora
- Timing of Surgery For Congenital Diaphragmatic Hernia: Is Emergency Operation Necessary?Documento4 pagineTiming of Surgery For Congenital Diaphragmatic Hernia: Is Emergency Operation Necessary?Agus PrimaNessuna valutazione finora
- 120 433 1 PBDocumento5 pagine120 433 1 PBNiaNessuna valutazione finora
- Early Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients A Randomised Controlled Trial - Barker2010Documento2 pagineEarly Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients A Randomised Controlled Trial - Barker2010RodrigoSachiFreitasNessuna valutazione finora
- Timing of Surgery in Traumatic Brachial Plexus Injury: A Systematic ReviewDocumento13 pagineTiming of Surgery in Traumatic Brachial Plexus Injury: A Systematic ReviewaliceNessuna valutazione finora
- Review 2021 Analgesia in Pancreatic ResectionDocumento9 pagineReview 2021 Analgesia in Pancreatic Resectionvalerio.messinaNessuna valutazione finora
- Cryoablation For The Palliation of Painful Bone Metastasis: A Systematic ReviewDocumento14 pagineCryoablation For The Palliation of Painful Bone Metastasis: A Systematic ReviewcontatoNessuna valutazione finora
- Anesthesia Management in Respiratory DepressionDocumento7 pagineAnesthesia Management in Respiratory DepressionGandita AnggoroNessuna valutazione finora
- Use of Repositioning in Pressure Ulcer PreventionDocumento6 pagineUse of Repositioning in Pressure Ulcer Preventionerickn8318uNessuna valutazione finora
- Medical Supplies - English Vocabulary: Term MeaningDocumento16 pagineMedical Supplies - English Vocabulary: Term MeaningedonaNessuna valutazione finora
- Gowning and Gloving (Gowning)Documento3 pagineGowning and Gloving (Gowning)Iza TugadeNessuna valutazione finora
- Article - Medical NegligenceDocumento4 pagineArticle - Medical NegligenceSimon RajNessuna valutazione finora
- Bologna Guidelines For Diagnosis and ManagementDocumento20 pagineBologna Guidelines For Diagnosis and ManagementTony HardianNessuna valutazione finora
- Acupunture For Small Animal Neurologic DisordersDocumento19 pagineAcupunture For Small Animal Neurologic DisordersJorge VergaraNessuna valutazione finora
- Health Care Solutions From America's Business Community: The Path Forward For U.S. Health ReformDocumento67 pagineHealth Care Solutions From America's Business Community: The Path Forward For U.S. Health ReformU.S. Chamber of CommerceNessuna valutazione finora
- Fernandez-Vega Eye InstituteDocumento16 pagineFernandez-Vega Eye InstituteFabricio Eric ParraNessuna valutazione finora
- Checklist For Review of Floor Plans Level 1Documento5 pagineChecklist For Review of Floor Plans Level 1jherica baltazarNessuna valutazione finora
- CATHDocumento10 pagineCATHPrasann RoyNessuna valutazione finora
- Tecnis Eyhance SpecSheetDocumento2 pagineTecnis Eyhance SpecSheetkesavan91Nessuna valutazione finora
- Open Journal of SurgeryDocumento6 pagineOpen Journal of SurgerySciresNessuna valutazione finora
- NCP Pain - ArthroDocumento6 pagineNCP Pain - ArthroKDnurseboyNessuna valutazione finora
- Aldaco Gender Modification SuitDocumento30 pagineAldaco Gender Modification SuitRob LauciusNessuna valutazione finora
- Jameson Chassin-Operative StrategyDocumento566 pagineJameson Chassin-Operative StrategyMaria Alexandra100% (3)
- Dental AnaesthesiaDocumento3 pagineDental AnaesthesiaSamer TarekNessuna valutazione finora
- Jurnal - PPT Total Hip ReplacementsDocumento11 pagineJurnal - PPT Total Hip ReplacementsEric GibsonNessuna valutazione finora
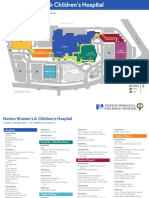
- NWCH Campus Map 1Documento2 pagineNWCH Campus Map 1Sara DiabNessuna valutazione finora
- JTCVS Information For Authors 2019 Revised 8-16-19Documento35 pagineJTCVS Information For Authors 2019 Revised 8-16-19irmelodyNessuna valutazione finora
- CM 86 192Documento4 pagineCM 86 192lucia pereiraNessuna valutazione finora
- (2021) Three-Flap Mastopexy With Reduction or AugmentationDocumento15 pagine(2021) Three-Flap Mastopexy With Reduction or AugmentationjlkjñklNessuna valutazione finora
- Appropriate Oral Health CareDocumento21 pagineAppropriate Oral Health CareSupriya BhataraNessuna valutazione finora
- Ayurveda and Modern Medice (A Critical Study) Kaviraj A.MajumdarDocumento13 pagineAyurveda and Modern Medice (A Critical Study) Kaviraj A.MajumdarShihan SilvaNessuna valutazione finora
- Ileal Pouches: Chapter 189: Supravesical Urinary DiversionDocumento1 paginaIleal Pouches: Chapter 189: Supravesical Urinary DiversioncesaliapNessuna valutazione finora
- Newsletter ISAPS May-August-2012 PDFDocumento21 pagineNewsletter ISAPS May-August-2012 PDFhuyenthanh1807Nessuna valutazione finora
- 194102-Article Text-491467-1-10-20200403Documento6 pagine194102-Article Text-491467-1-10-20200403mufcharovaNessuna valutazione finora
- [Journal of the American Veterinary Medical Association] Development of Enhanced Recovery After Surgery (ERAS) protocols in veterinary medicine through a one-health approach_ the role of anesthesia and locoregional techniquesDocumento9 pagine[Journal of the American Veterinary Medical Association] Development of Enhanced Recovery After Surgery (ERAS) protocols in veterinary medicine through a one-health approach_ the role of anesthesia and locoregional techniquesFrancisco Laecio Silva de AquinoNessuna valutazione finora
- Thesis Topics in General MedicineDocumento6 pagineThesis Topics in General MedicineCustomPaperServicesWashington100% (2)
- Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ)Documento17 pagineJapanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ)ishak_alsophNessuna valutazione finora
- Rise of Modern Surgery OrigiDocumento46 pagineRise of Modern Surgery OrigiPriyanka KaranamNessuna valutazione finora
- Fractal RobotsDocumento6 pagineFractal RobotsMonicaReddyNessuna valutazione finora




















































































![[Journal of the American Veterinary Medical Association] Development of Enhanced Recovery After Surgery (ERAS) protocols in veterinary medicine through a one-health approach_ the role of anesthesia and locoregional techniques](https://imgv2-1-f.scribdassets.com/img/document/597027379/149x198/4e86c3e723/1710567751?v=1)



