Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Fa Q Internship ProgramDocumento5 pagineFa Q Internship ProgramMariam A. KarimNessuna valutazione finora
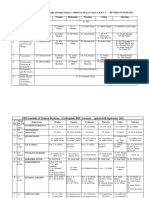
- Revised Schedule of BHU SSH OPD (Soft Copy) 2021Documento7 pagineRevised Schedule of BHU SSH OPD (Soft Copy) 2021rajubhagatssmNessuna valutazione finora
- Bai Tap Doc Hieu ChonDocumento27 pagineBai Tap Doc Hieu Chondungtran28041987Nessuna valutazione finora
- VaneDocumento16 pagineVanerafaelNessuna valutazione finora
- T20 Operating Table BrochureDocumento12 pagineT20 Operating Table BrochureCatur SetiawanNessuna valutazione finora
- Vicorder PWA-PWV Pres 15-04 EnglDocumento79 pagineVicorder PWA-PWV Pres 15-04 EnglHatem FaroukNessuna valutazione finora
- Doctor's DatabaseDocumento9 pagineDoctor's DatabaseMãçåbrê MähíNessuna valutazione finora
- PRC Forms Bicol University COllege of Nursing, Legazpi CityDocumento5 paginePRC Forms Bicol University COllege of Nursing, Legazpi CityekagaliasNessuna valutazione finora
- Cardiopulmonary Resuscitation: Unusual Techniques For Unusual Situations ConclusionDocumento8 pagineCardiopulmonary Resuscitation: Unusual Techniques For Unusual Situations ConclusionIlham AkbarNessuna valutazione finora
- Placing Piggy Back An Easy Way OutDocumento2 paginePlacing Piggy Back An Easy Way OutMawar Putri JulicaNessuna valutazione finora
- Ocala Medical CatalogDocumento9 pagineOcala Medical Catalogjeremy_ocala100% (1)
- Paederus Dermatitis An Outbreak On A Medical Mission AmazonDocumento3 paginePaederus Dermatitis An Outbreak On A Medical Mission AmazonrrrawNessuna valutazione finora
- Hematología - Williams (Tomo 1)Documento1.036 pagineHematología - Williams (Tomo 1)LIliana100% (3)
- Diagnostic Medical Sales Executive in Austin TX Resume Tom CollierDocumento2 pagineDiagnostic Medical Sales Executive in Austin TX Resume Tom CollierTomCollierNessuna valutazione finora
- Paranasal SinusDocumento51 pagineParanasal Sinusjosephwilliams_joeyNessuna valutazione finora
- College News Spring 2016Documento32 pagineCollege News Spring 2016AripinSyarifudinNessuna valutazione finora
- (Journal of Perinatal Medicine) Causes of Intrauterine Fetal Death Are Changing in Recent YearsDocumento5 pagine(Journal of Perinatal Medicine) Causes of Intrauterine Fetal Death Are Changing in Recent YearsGhea Jovita SinagaNessuna valutazione finora
- 2 2016MetabolicSyndromeComprehensiveTextbook2016GUODocumento880 pagine2 2016MetabolicSyndromeComprehensiveTextbook2016GUODewan Joheb Zaman50% (2)
- Devyani Lal, Peter H. Hwang - Frontal Sinus SurgeryDocumento442 pagineDevyani Lal, Peter H. Hwang - Frontal Sinus SurgeryHadi Mohammed Hamed67% (3)
- Medical AbbreviationsDocumento6 pagineMedical AbbreviationsEina CarmonaNessuna valutazione finora
- E-Book - Basic Concepts of PharmacokineticsDocumento71 pagineE-Book - Basic Concepts of PharmacokineticsCryslene VenancioNessuna valutazione finora
- Daftar Isi Paediatrica IndonesianaDocumento16 pagineDaftar Isi Paediatrica IndonesianaYURIS WIRDANessuna valutazione finora
- Contemporary Dental Pratice, 9 (3) :1-11.: Daftar PustakaDocumento4 pagineContemporary Dental Pratice, 9 (3) :1-11.: Daftar PustakaFasich BaihaqiNessuna valutazione finora
- PAVA-Riot Control AgentDocumento8 paginePAVA-Riot Control AgentLuděk SpurnýNessuna valutazione finora
- IV Fluid TherapyDocumento28 pagineIV Fluid Therapyansuh2250% (2)
- Hypnosis For Children Undergoing Dental TreatmentDocumento22 pagineHypnosis For Children Undergoing Dental TreatmentPuteri MentariNessuna valutazione finora
- PhimosisDocumento4 paginePhimosisHelvia Septarini TanjungNessuna valutazione finora
- APPENDIX A-Normal Values in HumansDocumento22 pagineAPPENDIX A-Normal Values in HumansSultan AlexandruNessuna valutazione finora
- Accident Investigation ProtocolsDocumento14 pagineAccident Investigation ProtocolsgilbertwildNessuna valutazione finora
- Distraction OsteogenesisDocumento28 pagineDistraction OsteogenesisManika SinghalNessuna valutazione finora