Chapter 7: Models for Working
with Psychiatric Patients
1 RECOVERY MODEL
Focus is on improving a persons competencies, not just alleviating symptoms
Movement toward a meaningful way of life; doesnt involve a cure
Patient strives to improve his or her own health and wellness
Striving to achieve full potential of life
Ten guiding principles:
o Person-drive
o Occurs via many pathways
o Holistic
o Supported by peers
o Supported through relationships
o Culturally based and influenced
o Supported by addressing trauma
o Strength-based
o Based on respect
o Emerges from hope
Collaborating with patients instead of telling them what to do
Encourage them to try new things
Patients take responsibility for their own care
Setbacks are not considered failures
Create atmosphere of hope
Person is not identified by his or her illness
Patients develop meaningful roles in their communities, not with the mental
health system
Support systems include family, peers, and community; peer support is
essential
Patient is incorporated in every level of planning, delivery, and evaluation of
mental services
2 PSYCHOANALYTICAL MODEL
Sigmund Freud: unconscious process of psychodynamic factors is the basis
for motivation and behavior
o Self-psychology: every human being longs to be appreciated
o Object relations theory: individuals relate to others based on
expectations formed by early experiences
If early parental relationships are secure and loving, the child grows up
secure in relationships
Disruptions in early parent-child relationships leads to future relationship
problems; distorts perceptions of others
Transference: unconscious distortion in the relationship; a patient displaces
distrustful feelings for her father onto her male psychiatrist and refuses
treatment
Projective identification: unconscious relationship-oriented mental
mechanism that when one person projects to the second person, who reacts
to the projection, the reaction elicits a response from the first person
2.1 CONSCIOUSNESS
Consciousness: material within a persons awareness
Unconsciousness: memories, conflicts, experiences, and material that have
been repressed and cannot be recalled at will
Preconsciousness: memories that can be recalled to the consciousness with
some effort
Insight into the meaning of symptoms facilitates change
2.2 DEFENSE MECHANISMS
When anxiety becomes too painful, defense mechanisms are used to protect
the ego and diminish anxiety
Excessive use prevent the person from problem solving
They are unconscious but some are within voluntary control
Denial: unconscious refusal to admit an unacceptable idea or behavior
Repression: unconscious and involuntary forgetting of painful ideas, events,
and conflicts
Suppression: conscious exclusion from awareness of anxiety-producing
feelings, ideas, and situations
Rationalization: conscious or unconscious attempts to justify ones feelings or
behaviors
Intellectualization: conscious or unconscious logical explanations without an
affective component
Dissociation: unconscious separation of painful feelings and emotions from an
unacceptable situation, object, or idea
Identification: conscious or unconscious attempt to model oneself after a
respected person
Introjection: unconsciously incorporating values and attitudes of others as if
they were your own
Compensation: consciously covering up for a weakness by overemphasizing
or making up a desirable trait
Sublimation: consciously or unconsciously channeling instinctual drives into
acceptable activities
Reaction formation: conscious behavior that is the exact opposite of an
unconscious feeling
Undoing: consciously doing something to counteract or make up for a
transgression
Displacement: unconsciously discharging pent-up feelings to a less
threatening object
Projection: unconsciously or consciously blaming someone else for ones
difficulties
Conversion: unconscious expression of intrapsychic conflict symbolically
through physical symptoms
Regression: unconscious return to an earlier more comfortable developmental
level
2.3 RELEVANCE
TO NURSING PRACTICE
Nurse must recognize and understand the maladaptive defense mechanisms,
share observations regarding the defense mechanisms, assist the patient to
increase their awareness of using the defense mechanisms, and increase the
use of adaptive behaviors
3 DEVELOPMENTAL MODEL
Eriksons theory: Every person must pass through eight interrelated stages
over the life cycle
Failure to complete a stage results in reduced ability to cope psychologically
Trust vs. Mistrust: (0-18 months) develop realistic trust of self and others
Autonomy vs. Shame (18 months 3 years) developing self-control and
willpower
Initiative vs. Guilt (3-5 years) developing an adequate conscience
Industry vs. Inferiority (6-12 years) sense of competence
Identity vs. Role (12-20 years) confident sense of self
Intimacy vs. Isolation (18-30 years) ability to give and receive love
Generative lifestyle vs. Stagnation (30-65 years) product, constructive,
and creative activity
Integrity vs. Despair (65-death) feelings of self-acceptance
3.1 RELEVANCE
TO NURSING PRACTICE
Patients with psychiatric disorders demonstrate partial mastery of
developmental stages
Nurses conduct assessment on the patients level of function to identify the
degree of mastery of each stage up to the patients age
Assessment reveals issues that need to be addressed while working with the
patient
4 INTERPERSONAL MODEL
Sullivan: believes that interactional is more important than intrapsychic
Healthy person: social being with ability to have relationships
Mental illness: lack of awareness or lack of skills in relationships
Relationships are viewed as sources of anxiety, maladaptive behavior, and
negative personality formation
Interpersonal psychotherapy (IPT): used for treatment of depression and
other mood disorders
o Addresses stressful social and interpersonal dynamics associated with
depressive symptoms
o Goal: improve social functioning by examining interpersonal disputes,
role transitions, grief, and interpersonal deficits
4.1 NURSES ROLE
Focus on current interpersonal relationships and experiences
Develop mature and satisfactory relationships relatively free from anxiety
Focus on interpersonal issues and distortions due to past experiences
Nurse corrects distortions with clear communication, consensual validation,
warm collaborative relationship
Present the patient as worthwhile and respect the patients rights, dignity,
and valuable abilities
Focus of sessions: loneliness, fear of rejection, clarifying emotions, using
anxiety to learn about self and other
Therapy is time limited, usually for 3 months
5 COGNITIVE BEHAVIORAL MODELS
Becks cognitive therapy and Ellis rational-emotive therapy models: focus on
thinking and behavior rather than on expressing feelings
Cognitive approach: ability to think, analyze, judge, decide, and do
Irrational and illogical beliefs are responsible for causing problems
Cognitive therapy: examines distorted perceptions by reality testing and
problem solving aimed at correcting the distorted processes
o Challenges the automatic thoughts to help patients develop logical
thoughts and feelings
o CBT: builds on cognitive therapy with learning principles
Motivational Enhancement Therapy: enhances the patients readiness and
willingness to change habits and relation to addictions using motivational
interviewing
Dialectical Behavioral Therapy: treats borderline personality disorder and
complex PTSD
o Decreases parasuicidal behavior of self-mutilation and suicidal
attempts
5.1 NURSES ROLE
Humor used to confront ineffective thinking
Focus on therapy is on the present
Patients learn to take responsibility for irrational thoughts, feelings, and
behavior to replace with more productive ones
Assist the patient to learn from mistakes
Patients who project blame are shown that theyre responsible for their
behaviors
Potrebbero piacerti anche
- Chapter 2 Lesson 3 Learning Input 1 2Documento26 pagineChapter 2 Lesson 3 Learning Input 1 2Myla Claire AlipioNessuna valutazione finora
- Therapeutic Modalities: Therapeutic Modalities, Psychosocial Skills, and Nursing 1 Biophysical/ Somatic InterventionsDocumento15 pagineTherapeutic Modalities: Therapeutic Modalities, Psychosocial Skills, and Nursing 1 Biophysical/ Somatic InterventionsdaliaNessuna valutazione finora
- Therapeutic Relationship - 2Documento45 pagineTherapeutic Relationship - 2Zaraki yami100% (1)
- C CEF Roles, Character, Team PlainDocumento10 pagineC CEF Roles, Character, Team PlainConrad C. CatimbangNessuna valutazione finora
- Nursing Care Plan: Angeles University Foundation College of NursingDocumento2 pagineNursing Care Plan: Angeles University Foundation College of NursingRey Ann PangilinanNessuna valutazione finora
- Cognitive Therapy Developed by Aaron T. Beck Focuses on Changing Faulty ThinkingDocumento7 pagineCognitive Therapy Developed by Aaron T. Beck Focuses on Changing Faulty Thinkingshivani singhNessuna valutazione finora
- Helping a Depressed Patient Cope with COVID-19Documento2 pagineHelping a Depressed Patient Cope with COVID-19Jenny Agustin FabrosNessuna valutazione finora
- Bachelor of Science in Nursing: Intensive Nursing Practicum: Rle LCP Module Rle LCP Unit WeekDocumento8 pagineBachelor of Science in Nursing: Intensive Nursing Practicum: Rle LCP Module Rle LCP Unit WeekMichelle Gliselle Guinto MallareNessuna valutazione finora
- Reflection Journal About SchizophreniaDocumento1 paginaReflection Journal About SchizophreniaKit LaraNessuna valutazione finora
- Introduction-: Post Traumatic Stress Disorder (PTSD)Documento10 pagineIntroduction-: Post Traumatic Stress Disorder (PTSD)preeti sharmaNessuna valutazione finora
- Therapeutic CommunicationDocumento3 pagineTherapeutic CommunicationPhilip Gene II Malacas100% (1)
- Self-Care: FirstDocumento2 pagineSelf-Care: FirstAllen KateNessuna valutazione finora
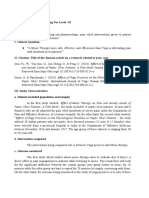
- The Ebn A. Evidence Based Nursing For Level III General QuestionDocumento7 pagineThe Ebn A. Evidence Based Nursing For Level III General QuestionAvyNessuna valutazione finora
- CASE PRESENTATION PP - Anxiety. Tiffany GordonDocumento6 pagineCASE PRESENTATION PP - Anxiety. Tiffany GordonTiffany GordonNessuna valutazione finora
- Mental Health Continuum ExplainedDocumento2 pagineMental Health Continuum ExplainedAileen A. MonaresNessuna valutazione finora
- 3 Determinants of LearningDocumento6 pagine3 Determinants of LearningKenNessuna valutazione finora
- Group NCPDocumento17 pagineGroup NCPNiña Noreen Torres VallegaNessuna valutazione finora
- Improved NutritionDocumento2 pagineImproved NutritionDaintyGarciaNessuna valutazione finora
- COPAR or Community Organizing Participatory Action Research Is A Vital Part ofDocumento5 pagineCOPAR or Community Organizing Participatory Action Research Is A Vital Part ofPrei BaltazarNessuna valutazione finora
- MseDocumento5 pagineMseYnaffit Alteza UntalNessuna valutazione finora
- ETIC211 Moral RelativismDocumento1 paginaETIC211 Moral RelativismNadineNessuna valutazione finora
- Nursing Care Plan for Alcohol Withdrawal AnxietyDocumento5 pagineNursing Care Plan for Alcohol Withdrawal Anxietykuro hanabusaNessuna valutazione finora
- Communication skills for mental health nursesDocumento15 pagineCommunication skills for mental health nursesKevin Leo Lucero AragonesNessuna valutazione finora
- Newborn Care ProceduresDocumento5 pagineNewborn Care Proceduresallkhusairy6tuansiNessuna valutazione finora
- Nursing Theorists and their Major ContributionsDocumento22 pagineNursing Theorists and their Major ContributionsG a i l R i c h w e l lNessuna valutazione finora
- NAME: Kristyn Joy D. Atangen: Subjective: DXDocumento5 pagineNAME: Kristyn Joy D. Atangen: Subjective: DXTyn TynNessuna valutazione finora
- Jenninngs Disaster Nursing Management Model Annotated BibliographyDocumento2 pagineJenninngs Disaster Nursing Management Model Annotated BibliographyEmergencyPlanning101Nessuna valutazione finora
- CHN Lecture Notes Module 3Documento4 pagineCHN Lecture Notes Module 3fallenNessuna valutazione finora
- Health History and Interview GuidelinesDocumento2 pagineHealth History and Interview GuidelinesGeraldine GonzalesNessuna valutazione finora
- Hebephrenic SchizophreniaDocumento2 pagineHebephrenic SchizophreniaJanelle Matamorosa100% (1)
- Nurse Patient RelationshipDocumento29 pagineNurse Patient Relationshipaseel jamalNessuna valutazione finora
- Nursing Care Plan for Postpartum Hemorrhage AnxietyDocumento2 pagineNursing Care Plan for Postpartum Hemorrhage AnxietyThe Right WayNessuna valutazione finora
- FNCP On Elevated Blood Pressure 2Documento4 pagineFNCP On Elevated Blood Pressure 2Aaron EspirituNessuna valutazione finora
- Role - Responsibilities of Psychiatry Health NurseDocumento3 pagineRole - Responsibilities of Psychiatry Health NurseDhAiRyA ArOrANessuna valutazione finora
- Therapeutic Communication in Psychiatric NursingDocumento7 pagineTherapeutic Communication in Psychiatric NursingKatrina BuenconsejoNessuna valutazione finora
- Termination PhaseDocumento2 pagineTermination PhaseDarlene LaudeNessuna valutazione finora
- Module 12Documento12 pagineModule 12mirai desuNessuna valutazione finora
- CHN - Written ReportDocumento3 pagineCHN - Written ReportJastine DiazNessuna valutazione finora
- Impact of Pandemic To The Psychological Aspects of Nursing StudentsDocumento25 pagineImpact of Pandemic To The Psychological Aspects of Nursing StudentsBrandon AreteNessuna valutazione finora
- Addressing The Stigma On Mental IllnessDocumento2 pagineAddressing The Stigma On Mental IllnessAubrey SungaNessuna valutazione finora
- Cues Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationDocumento2 pagineCues Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationAllana RayosNessuna valutazione finora
- NCM 117-Somatic DisordersDocumento5 pagineNCM 117-Somatic DisordersJa DimasNessuna valutazione finora
- Nursing Care Plan for ManiaDocumento1 paginaNursing Care Plan for ManiaJasmine BaduaNessuna valutazione finora
- Health Teaching Plan AMLDocumento2 pagineHealth Teaching Plan AMLInah Floresta BesasNessuna valutazione finora
- My Sister's KeeperDocumento3 pagineMy Sister's KeeperKirby ContaoiNessuna valutazione finora
- 1 Child Abuse Nursing Care Plan PDFDocumento7 pagine1 Child Abuse Nursing Care Plan PDFMAHESH KOUJALAGINessuna valutazione finora
- College of Nursing Case Study on Gestational DiabetesDocumento32 pagineCollege of Nursing Case Study on Gestational DiabetesRich-Anne LagarasNessuna valutazione finora
- Psychology Unit III PDFDocumento34 paginePsychology Unit III PDFOmprakash SwamiNessuna valutazione finora
- Self-Efficacy Strategies and Academic PerformanceDocumento20 pagineSelf-Efficacy Strategies and Academic PerformanceDianne Mae DagaNessuna valutazione finora
- Working With Groups Towards Community DevelopmentDocumento49 pagineWorking With Groups Towards Community DevelopmentUndine TapangNessuna valutazione finora
- Session 14: Common Humanity: Our Lady of Fatima University Veritas Et MisericordiaDocumento6 pagineSession 14: Common Humanity: Our Lady of Fatima University Veritas Et MisericordiaDarling Rose De GuzmanNessuna valutazione finora
- Teaching Care Plan STROKEDocumento2 pagineTeaching Care Plan STROKEKristine AbalosNessuna valutazione finora
- MS Case PresDocumento54 pagineMS Case PresShaine_Thompso_6877Nessuna valutazione finora
- Geriatric Depression ScaleDocumento2 pagineGeriatric Depression ScaleJess RitumaltaNessuna valutazione finora
- Paplau, AbdellahDocumento41 paginePaplau, AbdellahJ Ta RaNessuna valutazione finora
- Cultural Competence in NursingDocumento6 pagineCultural Competence in NursingAmiLia CandrasariNessuna valutazione finora
- Overview of Psychiatric NursingDocumento28 pagineOverview of Psychiatric Nursingjumar_ubalde1472Nessuna valutazione finora
- Nurse As A Profession Part IDocumento16 pagineNurse As A Profession Part IRuma Banerjee100% (1)
- CHN 1 Reg 8 HEALTH TEACHING PLAN FORMATDocumento2 pagineCHN 1 Reg 8 HEALTH TEACHING PLAN FORMATChristine SaliganNessuna valutazione finora
- Approaches To Counselling: by Amala Mary JohnyDocumento22 pagineApproaches To Counselling: by Amala Mary Johnyammu2805Nessuna valutazione finora
- Community As Partner - Chapter 10Documento7 pagineCommunity As Partner - Chapter 10KTNessuna valutazione finora
- Community As Partner - Chapter 5Documento1 paginaCommunity As Partner - Chapter 5KT0% (1)
- Community As Partner - Chapter 4Documento3 pagineCommunity As Partner - Chapter 4KT100% (1)
- Community As Partner - Chapter 2Documento2 pagineCommunity As Partner - Chapter 2KTNessuna valutazione finora
- Community As Partner - Chapter 6Documento2 pagineCommunity As Partner - Chapter 6KT0% (1)
- Chapter 13: Antiparkinsonian DrugsDocumento5 pagineChapter 13: Antiparkinsonian DrugsKT100% (1)
- Community As Partner - Chapter 3Documento4 pagineCommunity As Partner - Chapter 3KTNessuna valutazione finora
- Community As Partner - Chapter 1Documento5 pagineCommunity As Partner - Chapter 1KTNessuna valutazione finora
- Chapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersDocumento10 pagineChapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersKTNessuna valutazione finora
- Chapter 8 - Learning To Communicate ProfessionallyDocumento4 pagineChapter 8 - Learning To Communicate ProfessionallyKTNessuna valutazione finora
- Chapter 3 - Legal IssuesDocumento6 pagineChapter 3 - Legal IssuesKTNessuna valutazione finora
- Chapter 6 - Spiritual IssuesDocumento3 pagineChapter 6 - Spiritual IssuesKTNessuna valutazione finora
- Chapter 2 - Historical IssuesDocumento1 paginaChapter 2 - Historical IssuesKTNessuna valutazione finora
- Chapter 1 - Me, Meds, MilieuDocumento3 pagineChapter 1 - Me, Meds, MilieuKTNessuna valutazione finora
- Student Teacher Performance Everett Pickleball 1Documento2 pagineStudent Teacher Performance Everett Pickleball 1api-302193708Nessuna valutazione finora
- English Teaching in Indonesia SoenjonoDocumento9 pagineEnglish Teaching in Indonesia SoenjonoEryansyah NasirNessuna valutazione finora
- Final Curriculum Implementation Matrix Cim World ReligionDocumento5 pagineFinal Curriculum Implementation Matrix Cim World ReligionBaby YanyanNessuna valutazione finora
- 1Documento2 pagine1Khan KhanNessuna valutazione finora
- Individual Learning Monitoring PlanDocumento2 pagineIndividual Learning Monitoring PlanJimwel GutierrezNessuna valutazione finora
- Test Bank For Social Psychology 5th Edition Tom GilovichDocumento13 pagineTest Bank For Social Psychology 5th Edition Tom GilovichDevin MckayNessuna valutazione finora
- Sample Quali ASMR - ManuscriptDocumento26 pagineSample Quali ASMR - ManuscriptKirzten Avril R. AlvarezNessuna valutazione finora
- Patterns Grade 1Documento5 paginePatterns Grade 1kkgreubelNessuna valutazione finora
- The Reading The Mind in The Eyes TestDocumento13 pagineThe Reading The Mind in The Eyes TestMonaNessuna valutazione finora
- Eapp Lesson 1Documento42 pagineEapp Lesson 1angelicaNessuna valutazione finora
- IIAS Newsletter 2020 EditionDocumento16 pagineIIAS Newsletter 2020 EditionOgunoyeOladimejiRaphaelNessuna valutazione finora
- CEFR Mapping: Level: B1 A World of DifferenceDocumento13 pagineCEFR Mapping: Level: B1 A World of DifferenceElisabete BentivenhaNessuna valutazione finora
- VAPA CurriculumDocumento232 pagineVAPA Curriculumroxanna_mohammedNessuna valutazione finora
- Detecting Stress Based On Social Interactions in Social NetworksDocumento4 pagineDetecting Stress Based On Social Interactions in Social NetworksAstakala Suraj Rao100% (1)
- English: Quarter 2 - Module 7: A Venture To The Wonders of Reading and ListeningDocumento32 pagineEnglish: Quarter 2 - Module 7: A Venture To The Wonders of Reading and ListeningMercy GanasNessuna valutazione finora
- English Phrases For Meetings - Espresso EnglishDocumento8 pagineEnglish Phrases For Meetings - Espresso Englishasamwm.english1Nessuna valutazione finora
- The Different Types of Speech Context and Speech StyleDocumento2 pagineThe Different Types of Speech Context and Speech StyleaquelaNessuna valutazione finora
- Quiz Introduction To SCRUMDocumento3 pagineQuiz Introduction To SCRUMr076755a0% (1)
- Questionnaire Life Long Learners With 21ST Century Skills PDFDocumento3 pagineQuestionnaire Life Long Learners With 21ST Century Skills PDFHenry Buemio0% (1)
- Week 2 EIM 12 Q1 Indoyon Evaluated ESDocumento8 pagineWeek 2 EIM 12 Q1 Indoyon Evaluated ESMarino L. SanoyNessuna valutazione finora
- Psychology 2012Documento49 paginePsychology 2012Tom AldertonNessuna valutazione finora
- Edu 214 - Assignment 1Documento2 pagineEdu 214 - Assignment 1api-594749217Nessuna valutazione finora
- Afro AsianDocumento18 pagineAfro AsiangraceNessuna valutazione finora
- Writing ObjectivesDocumento32 pagineWriting ObjectivesTita RakhmitaNessuna valutazione finora
- A Long EssayDocumento2 pagineA Long EssaysunnybakliwalNessuna valutazione finora
- Semantics exam questions and answersDocumento4 pagineSemantics exam questions and answersThiên Huy100% (1)
- Maria Montessori: My System of EducationDocumento36 pagineMaria Montessori: My System of EducationAnaisisiNessuna valutazione finora
- Conceptual FrameworkDocumento7 pagineConceptual Framework'AcqhoziihFamousxzSzupfisxzticqkeiytEdNessuna valutazione finora
- Reading: Rowell de Guia Bataan Peninsula State UniversityDocumento16 pagineReading: Rowell de Guia Bataan Peninsula State UniversityRojane FloraNessuna valutazione finora
- Chapter 11: Prognosis and Treatment PlanningDocumento10 pagineChapter 11: Prognosis and Treatment PlanningNikiNessuna valutazione finora