Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
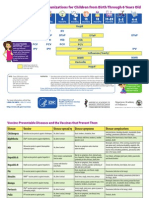
- 04 Immunizations and Developmental Milestones For Your Child From Birth Through 6 Years OldDocumento2 pagine04 Immunizations and Developmental Milestones For Your Child From Birth Through 6 Years Oldapi-309082881Nessuna valutazione finora
- FNCPDocumento3 pagineFNCPLander VirayNessuna valutazione finora
- Pregnancy Following Miscarriage What Is The Optimum Interpregnancy IntervalDocumento3 paginePregnancy Following Miscarriage What Is The Optimum Interpregnancy IntervallcmurilloNessuna valutazione finora
- ACOG Practice Advisory On Annual Pelvic Examination RecommendationsDocumento1 paginaACOG Practice Advisory On Annual Pelvic Examination RecommendationslcmurilloNessuna valutazione finora
- Everyday Contraception ConsiderationsDocumento15 pagineEveryday Contraception ConsiderationslcmurilloNessuna valutazione finora
- Caffeine Intake - Even Dad's - Linked To Miscarriage, Study Says - MedlinePlusDocumento3 pagineCaffeine Intake - Even Dad's - Linked To Miscarriage, Study Says - MedlinePluslcmurilloNessuna valutazione finora
- Patient-Centered Risk Assessment For Ovarian CancerDocumento13 paginePatient-Centered Risk Assessment For Ovarian CancerlcmurilloNessuna valutazione finora
- Obgm Feb2018 Vol.30 No.2 PDFDocumento55 pagineObgm Feb2018 Vol.30 No.2 PDFlcmurilloNessuna valutazione finora
- Alteration of The Hormone-Free IntervalDocumento2 pagineAlteration of The Hormone-Free IntervalAnonymous d4X4wZLDNessuna valutazione finora
- Obgm Mar2018 Vol.30 No.3Documento57 pagineObgm Mar2018 Vol.30 No.3lcmurilloNessuna valutazione finora
- Obgm Mar2018 Vol.30 No.3Documento57 pagineObgm Mar2018 Vol.30 No.3lcmurilloNessuna valutazione finora
- A Randomized Trial Comparing SkinDocumento9 pagineA Randomized Trial Comparing SkinlcmurilloNessuna valutazione finora
- Obgm Modern Day Laboring FinalDocumento8 pagineObgm Modern Day Laboring FinallcmurilloNessuna valutazione finora
- Pelvic Examination 3Documento1 paginaPelvic Examination 3lcmurilloNessuna valutazione finora
- Pelvic ExaminationDocumento14 paginePelvic ExaminationlcmurilloNessuna valutazione finora
- HBV Screening 5Documento3 pagineHBV Screening 5lcmurilloNessuna valutazione finora
- HBV ScreeningDocumento24 pagineHBV ScreeninglcmurilloNessuna valutazione finora
- HBV Screening 4Documento1 paginaHBV Screening 4lcmurilloNessuna valutazione finora
- Pelvic Examination 2Documento7 paginePelvic Examination 2lcmurilloNessuna valutazione finora
- HBV Screening 2Documento10 pagineHBV Screening 2lcmurilloNessuna valutazione finora
- 11complications of Unsafe Abortion in Sub-SaharanDocumento15 pagine11complications of Unsafe Abortion in Sub-SaharanlcmurilloNessuna valutazione finora
- P 4065Documento2 pagineP 4065lcmurilloNessuna valutazione finora
- Pi Is 074937970300120 XDocumento7 paginePi Is 074937970300120 XlcmurilloNessuna valutazione finora
- P 4036Documento3 pagineP 4036lcmurilloNessuna valutazione finora
- 2013 Recommended Adolescent ImmunizationDocumento2 pagine2013 Recommended Adolescent ImmunizationArvi MandaweNessuna valutazione finora
- P 4060Documento2 pagineP 4060lcmurilloNessuna valutazione finora
- Catchup ScheduleDocumento4 pagineCatchup ScheduleAisha SyedNessuna valutazione finora
- Parent Ver SCH 0 6yrsDocumento2 pagineParent Ver SCH 0 6yrslcmurilloNessuna valutazione finora
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Documento4 pagineSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)gyna_2002Nessuna valutazione finora
- Biosensors 12 00985 v2Documento30 pagineBiosensors 12 00985 v2aqsa javedNessuna valutazione finora
- Nebulizing & Suctioning TechniquesDocumento23 pagineNebulizing & Suctioning TechniquesRifky Octavio PNessuna valutazione finora
- IM STEP 2 NotesDocumento74 pagineIM STEP 2 Notesyanks1120100% (3)
- SepanskiDocumento13 pagineSepanskiTammy Utami DewiNessuna valutazione finora
- Internet Gaming Disorder Among AdolescentsDocumento10 pagineInternet Gaming Disorder Among AdolescentsGurumoorthy Dr.SureshkumarNessuna valutazione finora
- Option Volume Ventilation Pi 9066364 en 1506 3Documento2 pagineOption Volume Ventilation Pi 9066364 en 1506 3Abdullah AlsafiNessuna valutazione finora
- Supplement-1115 2020Documento216 pagineSupplement-1115 2020Laura PaunicaNessuna valutazione finora
- Information and Resources For Effective Self-Management of Problem Substance UseDocumento52 pagineInformation and Resources For Effective Self-Management of Problem Substance Useedmidler100% (1)
- Web KFOG-jan-11Documento16 pagineWeb KFOG-jan-11kutra3000Nessuna valutazione finora
- RADIOLOGYDocumento3 pagineRADIOLOGYwendy carinoNessuna valutazione finora
- Aneroxia Research PaperDocumento34 pagineAneroxia Research PaperDuaa HammadNessuna valutazione finora
- Simplicity and Versatility: Philips Respironics Trilogy 202 Portable Ventilator SpecificationsDocumento4 pagineSimplicity and Versatility: Philips Respironics Trilogy 202 Portable Ventilator SpecificationsVincent Seow Youk EngNessuna valutazione finora
- Drug Tabulation orDocumento23 pagineDrug Tabulation orChin Villanueva UlamNessuna valutazione finora
- Loneliness and Social Isolation in Older Adults-The Effects of A PandemicDocumento8 pagineLoneliness and Social Isolation in Older Adults-The Effects of A Pandemicmadalena limaNessuna valutazione finora
- Integrated Management of Childhood Illnes1Documento5 pagineIntegrated Management of Childhood Illnes1Ryan VocalanNessuna valutazione finora
- MSB Viewing Guide - 0102Documento4 pagineMSB Viewing Guide - 0102Jess WestwoodNessuna valutazione finora
- The Lightning-Fast Quest For COVID Vaccines - and What It Means For Other DiseasesDocumento3 pagineThe Lightning-Fast Quest For COVID Vaccines - and What It Means For Other DiseasesKathiravan M NNessuna valutazione finora
- Isicem 2021Documento90 pagineIsicem 2021labbeneNessuna valutazione finora
- Marasmus: An Update and Review of Literature: JSM Nutritional DisordersDocumento15 pagineMarasmus: An Update and Review of Literature: JSM Nutritional DisordersShanya rahma AdrianiNessuna valutazione finora
- Reaksi Hipersensitivitas Atau Alergi: RiwayatiDocumento7 pagineReaksi Hipersensitivitas Atau Alergi: Riwayatiaulia nissaNessuna valutazione finora
- AR 40-8 Effective 16 June 2007Documento10 pagineAR 40-8 Effective 16 June 2007kbin3838Nessuna valutazione finora
- Ultrasound-Guided Brachial Plexus BlockDocumento7 pagineUltrasound-Guided Brachial Plexus BlockÇağdaş BaytarNessuna valutazione finora
- Chapter 4 A1 Poster Example 2Documento3 pagineChapter 4 A1 Poster Example 2Krisna PamungkasNessuna valutazione finora
- UNAIDS Core Epidemiology Slides enDocumento11 pagineUNAIDS Core Epidemiology Slides enTabarcea VitaliNessuna valutazione finora
- Daftar 79 Jenis Alkes Yang Tidak Boleh DiimporDocumento1 paginaDaftar 79 Jenis Alkes Yang Tidak Boleh DiimporTaufik RiansyahNessuna valutazione finora
- CostipitationDocumento4 pagineCostipitationashmi akberNessuna valutazione finora
- Resusciation Equipments in IcuDocumento29 pagineResusciation Equipments in Icuvinoli100% (1)
- OSCE Subcutaneous Injection SkillsDocumento2 pagineOSCE Subcutaneous Injection SkillsvishnuNessuna valutazione finora
- CT ScanDocumento37 pagineCT ScanBayu Ihkshan Yamada TriatmojoNessuna valutazione finora