Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Traumatic Tympanic PerforationDocumento14 pagineTraumatic Tympanic PerforationNatalia CvNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Relacion Del Nervio Facial Con El Anillo TimpánicoDocumento4 pagineRelacion Del Nervio Facial Con El Anillo TimpánicoNatalia CvNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Audiometry Screening and InterpretationDocumento2 pagineAudiometry Screening and InterpretationNatalia CvNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Kdigo-Anemia and CKDDocumento64 pagineKdigo-Anemia and CKDn_catalinNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- KDIGO AKI Guideline DownloadDocumento141 pagineKDIGO AKI Guideline DownloadSandi AuliaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Skin Surgical Preparation Agents1Documento6 pagineSkin Surgical Preparation Agents1Natalia CvNessuna valutazione finora
- Acute Pulmonary Embolism ESC 2014Documento48 pagineAcute Pulmonary Embolism ESC 2014Diego Fernando Ortiz TenorioNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Adolescents and Long Acting Contraceptives ACOGDocumento7 pagineAdolescents and Long Acting Contraceptives ACOGNatalia CvNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Chestpain Care Clinical GuideDocumento13 pagineChestpain Care Clinical GuideNatalia CvNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Chestpain Care Clinical GuideDocumento13 pagineChestpain Care Clinical GuideNatalia CvNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- GOLD Pocket Guide 2014 COPDDocumento32 pagineGOLD Pocket Guide 2014 COPDNatalia CvNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- jnc8 PDFDocumento14 paginejnc8 PDFRizki NovitasariNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Ada 2014 PDFDocumento67 pagineAda 2014 PDFashmctqNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- Cyto 2.5Documento4 pagineCyto 2.5Medtech SoonNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Chapter 6: Cell Division: 6.3: MEIOSISDocumento29 pagineChapter 6: Cell Division: 6.3: MEIOSISMohammed RidzuwanNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Department of Molecular Virology: COVID-19 (Corona) VirusDocumento1 paginaDepartment of Molecular Virology: COVID-19 (Corona) VirusMuaaz ButtNessuna valutazione finora
- Interpreting human pedigreesDocumento3 pagineInterpreting human pedigreesmowehe4417Nessuna valutazione finora
- G8 Biology Lesson 2 Heredity Inheritance and Variation of TraitsDocumento2 pagineG8 Biology Lesson 2 Heredity Inheritance and Variation of TraitsCindy CrahayNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- GenPop 2 - Pola Pewarisan SifatDocumento29 pagineGenPop 2 - Pola Pewarisan SifatMonicha Yhuyhen SafitriNessuna valutazione finora
- Personal Philosophy of NursingDocumento5 paginePersonal Philosophy of NursingsarahreyNessuna valutazione finora
- Plants & Animals Reproduce Through Sexual & Asexual MethodsDocumento14 paginePlants & Animals Reproduce Through Sexual & Asexual MethodsAleli Joy Profugo DalisayNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- GC-MS Analysis of Nigella Sativa Seed Extract and Its Ameliorative Effects On Transgenic Drosophila Model of Parkinson DiseaseDocumento7 pagineGC-MS Analysis of Nigella Sativa Seed Extract and Its Ameliorative Effects On Transgenic Drosophila Model of Parkinson DiseaseInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- 1.6 Cell Division:mitosisDocumento3 pagine1.6 Cell Division:mitosisAzahra SaptoroNessuna valutazione finora
- Laguna University Midterm Exam in Natural Science IIDocumento3 pagineLaguna University Midterm Exam in Natural Science IIVinlax ArguillesNessuna valutazione finora
- Biopharmaceuticals Availability, Diffusion, Sustainability: Massimo Riccaboni University of Florence & CERM, RomeDocumento28 pagineBiopharmaceuticals Availability, Diffusion, Sustainability: Massimo Riccaboni University of Florence & CERM, RomeNoor hossainNessuna valutazione finora
- 2019 - Using Genetically Incorporated Unnatural AminoDocumento30 pagine2019 - Using Genetically Incorporated Unnatural AminodymscientificNessuna valutazione finora
- Speciation Natural Processes, Genetics and BiodiversityDocumento276 pagineSpeciation Natural Processes, Genetics and BiodiversityCristian BarrosNessuna valutazione finora
- (PDF) GenBio2 - Module - Week06Documento40 pagine(PDF) GenBio2 - Module - Week06Ramon Villota100% (1)
- Evolution: Is Change in The Heritable Characteristics of Biological Populations Over Successive GenerationsDocumento19 pagineEvolution: Is Change in The Heritable Characteristics of Biological Populations Over Successive GenerationsIyomi Faye De LeonNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Degree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentDocumento24 pagineDegree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentRJ DealcaNessuna valutazione finora
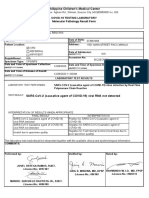
- Philippine Children's Medical Center: Covid-19 Testing Laboratory Molecular Pathology Result FormDocumento1 paginaPhilippine Children's Medical Center: Covid-19 Testing Laboratory Molecular Pathology Result FormRica RegorisNessuna valutazione finora
- Midterm Examihation, I (Ovember: PUC RrorDocumento2 pagineMidterm Examihation, I (Ovember: PUC Rrorjäšħwâñtħ rNessuna valutazione finora
- Biology Book For 9th ClassDocumento7 pagineBiology Book For 9th ClassSidra TulmuntahaNessuna valutazione finora
- Chapter III Pathopysiology (Print!!!)Documento3 pagineChapter III Pathopysiology (Print!!!)Kismet SummonsNessuna valutazione finora
- Report: Ranbaxy & Daiichi Sankyo Co. Ltd. Merger: BackgroundDocumento4 pagineReport: Ranbaxy & Daiichi Sankyo Co. Ltd. Merger: BackgroundAlaka DebtaNessuna valutazione finora
- Kromosom X D. Melanogaster. Skripsi Tidak Diterbitkan. Malang: IKIP MalangDocumento2 pagineKromosom X D. Melanogaster. Skripsi Tidak Diterbitkan. Malang: IKIP MalangMochab HafidhNessuna valutazione finora
- High Content ScreeningDocumento10 pagineHigh Content Screeningdevesh.hsNessuna valutazione finora
- Polymerase Chain Reaction (PCR)Documento37 paginePolymerase Chain Reaction (PCR)PRUDHVIAZADNessuna valutazione finora
- BIOTECHNOLOGY SYLLABUS AND COURSE STRUCTUREDocumento7 pagineBIOTECHNOLOGY SYLLABUS AND COURSE STRUCTURESheetal RajawatNessuna valutazione finora
- 6 Enzymes and Cellular Regulation-SDocumento5 pagine6 Enzymes and Cellular Regulation-Sapi-502781581Nessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- RingwormDocumento324 pagineRingwormRizky GumelarNessuna valutazione finora
- Diagnosis and Treatment of Kaposi SarcomaDocumento11 pagineDiagnosis and Treatment of Kaposi SarcomaSantiago Pedro Medina LópezNessuna valutazione finora
- Genetic Organization HandoutDocumento8 pagineGenetic Organization HandoutConnorNessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (402)