Potrebbero piacerti anche
- 03 Gait Mechanics&Deviations SummaryDocumento3 pagine03 Gait Mechanics&Deviations SummaryC Martin TraumatoNessuna valutazione finora
- Closed Traccion y EnyesadoDocumento64 pagineClosed Traccion y EnyesadoC Martin TraumatoNessuna valutazione finora
- Art 03Documento15 pagineArt 03C Martin TraumatoNessuna valutazione finora
- Management of Acute and Chronic Ankle InstabilityDocumento8 pagineManagement of Acute and Chronic Ankle InstabilityC Martin TraumatoNessuna valutazione finora
- Dislocation After Total Hip Arthroplasty - Implant Design and OrientationDocumento11 pagineDislocation After Total Hip Arthroplasty - Implant Design and OrientationC Martin TraumatoNessuna valutazione finora
- FF Re SpacerDocumento48 pagineFF Re SpacerC Martin TraumatoNessuna valutazione finora
- J. Antimicrob. Chemother. 2004 Bertazzoni Minelli 329 34Documento6 pagineJ. Antimicrob. Chemother. 2004 Bertazzoni Minelli 329 34C Martin TraumatoNessuna valutazione finora
- Intramedullary NailsDocumento51 pagineIntramedullary NailsC Martin TraumatoNessuna valutazione finora
- Intramedullary NailsDocumento51 pagineIntramedullary NailsC Martin TraumatoNessuna valutazione finora
- Flatfoot Deformity in Children and Adolescents - Surgical Indications and ManagementDocumento10 pagineFlatfoot Deformity in Children and Adolescents - Surgical Indications and ManagementC Martin TraumatoNessuna valutazione finora
- Brodie'S Abscess Revisited: Key-Word: Bones, AbscessDocumento6 pagineBrodie'S Abscess Revisited: Key-Word: Bones, AbscessC Martin TraumatoNessuna valutazione finora
- Fractures Radial Head & Neck. JBJS. 2013Documento10 pagineFractures Radial Head & Neck. JBJS. 2013C Martin TraumatoNessuna valutazione finora
- Ankle Syndesmotic InjuryDocumento10 pagineAnkle Syndesmotic InjuryC Martin TraumatoNessuna valutazione finora
- ConstreñidosDocumento10 pagineConstreñidosCelest ReyesNessuna valutazione finora
- Arthrodesis (Upper Extremity)Documento1 paginaArthrodesis (Upper Extremity)C Martin TraumatoNessuna valutazione finora
- Arthrodesis Techniques in The Management of Stage II and III Acquired Adult Flatfoot Deformity.Documento12 pagineArthrodesis Techniques in The Management of Stage II and III Acquired Adult Flatfoot Deformity.C Martin TraumatoNessuna valutazione finora
- Adult-Acquired Flatfoot DeformityDocumento8 pagineAdult-Acquired Flatfoot DeformityC Martin TraumatoNessuna valutazione finora
- Gandhi OrthoDocumento113 pagineGandhi OrthoC Martin TraumatoNessuna valutazione finora
- Pelvic OsteotomiesDocumento26 paginePelvic OsteotomiesC Martin TraumatoNessuna valutazione finora
- Displasia Bilateral Cadera BnoDocumento9 pagineDisplasia Bilateral Cadera BnoC Martin TraumatoNessuna valutazione finora
- Femoral Nerve Block For Diaphyseal and Distal Femoral Fractures in The Emergency DepartmentDocumento9 pagineFemoral Nerve Block For Diaphyseal and Distal Femoral Fractures in The Emergency DepartmentC Martin TraumatoNessuna valutazione finora
- Cabeza FemoralDocumento5 pagineCabeza FemoralC Martin TraumatoNessuna valutazione finora
- Pelvic OsteotomiesDocumento26 paginePelvic OsteotomiesC Martin TraumatoNessuna valutazione finora
- Alargamiento Del Complejo Gastronemio SoleoDocumento8 pagineAlargamiento Del Complejo Gastronemio SoleoC Martin TraumatoNessuna valutazione finora
- TotalHip PDFDocumento11 pagineTotalHip PDFC Martin TraumatoNessuna valutazione finora
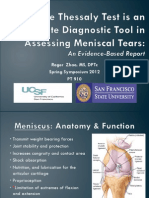
- Is the Thessaly Test an accurate examination tool for diagnosing meniscal tearsDocumento52 pagineIs the Thessaly Test an accurate examination tool for diagnosing meniscal tearsC Martin Traumato100% (2)
- Clavo Expert LFN Diafisis FemurDocumento84 pagineClavo Expert LFN Diafisis FemurC Martin TraumatoNessuna valutazione finora
- IHDI Ortho Presentation WebDocumento7 pagineIHDI Ortho Presentation WebC Martin TraumatoNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Module 1: Disability, Inequality, and InclusionDocumento25 pagineModule 1: Disability, Inequality, and InclusionAuberon Jeleel OdoomNessuna valutazione finora
- Patient Examination: History: by Professor of Internal MedicineDocumento47 paginePatient Examination: History: by Professor of Internal MedicineMonqith YousifNessuna valutazione finora
- Study On The Incidence of Urinary Tract Infections, Organisms Causing It and Antibiotic Susceptibility in Patients With DIABETES MELLITUS IN AJIMS, MLORE" For The Registration of Dissertation To RajivDocumento26 pagineStudy On The Incidence of Urinary Tract Infections, Organisms Causing It and Antibiotic Susceptibility in Patients With DIABETES MELLITUS IN AJIMS, MLORE" For The Registration of Dissertation To RajivR Hari0% (1)
- Aunt Minnie Pediatric NeuroDocumento15 pagineAunt Minnie Pediatric NeuroRommel OliverasNessuna valutazione finora
- Optimizing Active Case-Finding For Tuberculosis: Implementation Lessons From South-East AsiaDocumento97 pagineOptimizing Active Case-Finding For Tuberculosis: Implementation Lessons From South-East AsiaRisdi PramestaNessuna valutazione finora
- Department of General Surgery: Thermal Injuries Skin Grafts Acute AbdomenDocumento115 pagineDepartment of General Surgery: Thermal Injuries Skin Grafts Acute AbdomenAj Christian Lacuesta IsipNessuna valutazione finora
- Standards For Sanitation: What, Why and How?: Kate Hurley, DVM, MPVMDocumento26 pagineStandards For Sanitation: What, Why and How?: Kate Hurley, DVM, MPVMKaren SalcedoNessuna valutazione finora
- Chronic IllnessDocumento13 pagineChronic IllnessAnusha KumarasiriNessuna valutazione finora
- Product B - Edhawa Herbal MedicineDocumento3 pagineProduct B - Edhawa Herbal MedicineJae Tuffie KatneesNessuna valutazione finora
- Hypo Glice MiaDocumento13 pagineHypo Glice MiaNurul AmaliaNessuna valutazione finora
- Aortic AneurysmDocumento26 pagineAortic Aneurysmchetanm2563100% (1)
- EITC HSE Qualifications CalendarDocumento15 pagineEITC HSE Qualifications Calendarm_othman_4Nessuna valutazione finora
- Introduction To Practical Food Production 2019Documento16 pagineIntroduction To Practical Food Production 2019Quoc KhanhNessuna valutazione finora
- Liver Cirrhosis: Causes, Complications and ManagementDocumento55 pagineLiver Cirrhosis: Causes, Complications and ManagementAnonymous vUEDx8100% (1)
- Major Bioethical PrinciplesDocumento44 pagineMajor Bioethical PrinciplesDr. Liza Manalo50% (2)
- Dance Sports Workshop Activity ProposalDocumento3 pagineDance Sports Workshop Activity ProposalAya Sismondo100% (1)
- Osteomyelitis: Osteomyelitis Is Infection in The Bone. Osteomyelitis Can Occur in InfantsDocumento4 pagineOsteomyelitis: Osteomyelitis Is Infection in The Bone. Osteomyelitis Can Occur in Infantstiban_07Nessuna valutazione finora
- MediCover Student Medical InsuranceDocumento28 pagineMediCover Student Medical InsuranceNhung LuuNessuna valutazione finora
- Study of Incidence and Risk Factors For Surgical Site Infection After Cesarean Section at First Referral UnitDocumento3 pagineStudy of Incidence and Risk Factors For Surgical Site Infection After Cesarean Section at First Referral UnitFaozan FikriNessuna valutazione finora
- Neonatal Glycaemia and Neurodevelopmental Outcomes A Systematic Review and Meta Analysis.Documento11 pagineNeonatal Glycaemia and Neurodevelopmental Outcomes A Systematic Review and Meta Analysis.Alma Iris Rodriguez D PadillaNessuna valutazione finora
- Soal Lokasi KIK - 2Documento2 pagineSoal Lokasi KIK - 2novida nainggolanNessuna valutazione finora
- Homeopathy CuresDocumento18 pagineHomeopathy CureschampakNessuna valutazione finora
- Is An Intensive Outpatient ProgramDocumento1 paginaIs An Intensive Outpatient ProgramJack williamNessuna valutazione finora
- GGGDGGDocumento414 pagineGGGDGGOtiosse MyosotisNessuna valutazione finora
- Twisted Risk Assesment 2Documento2 pagineTwisted Risk Assesment 2api-306671250100% (1)
- Bipolar Disorder Symptoms, Causes and TreatmentDocumento108 pagineBipolar Disorder Symptoms, Causes and TreatmentMaica LectanaNessuna valutazione finora
- Clinico-Pathological Review On Pravahika Vis-A-Vis AmoebiasisDocumento3 pagineClinico-Pathological Review On Pravahika Vis-A-Vis AmoebiasisAdvanced Research PublicationsNessuna valutazione finora
- Eng QP FormatDocumento15 pagineEng QP Formatpriyansh asnaniNessuna valutazione finora
- Making Decisions About CPR: Learning OutcomesDocumento8 pagineMaking Decisions About CPR: Learning Outcomesicen00bNessuna valutazione finora
- Pai NMJI 2004 Systematic Reviews Illustrated Guide3Documento10 paginePai NMJI 2004 Systematic Reviews Illustrated Guide3mphil.rameshNessuna valutazione finora