Potrebbero piacerti anche
- Practice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaDocumento28 paginePractice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaRully SyahrizalNessuna valutazione finora
- Supraventricular Arrhythmias - Classificaiton, Etiology, ECG, Clinical Characteristics, TreatmentDocumento2 pagineSupraventricular Arrhythmias - Classificaiton, Etiology, ECG, Clinical Characteristics, TreatmentSoleNessuna valutazione finora
- A. Flutter, AFDocumento80 pagineA. Flutter, AFclaimstudent3515Nessuna valutazione finora
- Atrial RhythmDocumento12 pagineAtrial RhythmCarlo Domingo LadieroNessuna valutazione finora
- Neo Pedia Guidelines Arrhythmia PDFDocumento16 pagineNeo Pedia Guidelines Arrhythmia PDFkhludNessuna valutazione finora
- Narrow QRS Complex Tachycardias: Clinical Manifestations, Diagnosis, and EvaluatDocumento24 pagineNarrow QRS Complex Tachycardias: Clinical Manifestations, Diagnosis, and EvaluataspxxNessuna valutazione finora
- Supraventricular TachycardiaDocumento5 pagineSupraventricular TachycardialjubodragNessuna valutazione finora
- ECG HRV Assignment 19334107Documento18 pagineECG HRV Assignment 19334107katehughes332Nessuna valutazione finora
- Guar Raci No 2016Documento14 pagineGuar Raci No 2016ema moralesNessuna valutazione finora
- Lewis: Medical-Surgical Nursing, 8th Edition: Chapter 36: Nursing Management: Dysrhythmias Key Points - PrintableDocumento6 pagineLewis: Medical-Surgical Nursing, 8th Edition: Chapter 36: Nursing Management: Dysrhythmias Key Points - Printablelpirman05Nessuna valutazione finora
- Atrial Fibrillation (A Fib) OverviewDocumento11 pagineAtrial Fibrillation (A Fib) OverviewCory Monica MarpaungNessuna valutazione finora
- Arrhythmias PDFDocumento29 pagineArrhythmias PDFbencleeseNessuna valutazione finora
- Journal of Nursing: Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyDocumento8 pagineJournal of Nursing: Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyNiala AlmarioNessuna valutazione finora
- Aortic Stenosis AmendillaDocumento31 pagineAortic Stenosis AmendillaVadim BursacovschiNessuna valutazione finora
- Af 1Documento22 pagineAf 1muthiaraNessuna valutazione finora
- Broadly DefinedDocumento10 pagineBroadly DefinedJayvee AguilarNessuna valutazione finora
- Arrhythmia OF THE HEARTDocumento4 pagineArrhythmia OF THE HEARTSellappan MuthusamyNessuna valutazione finora
- Cardiac ArrythmiaDocumento16 pagineCardiac ArrythmiaHossen AliNessuna valutazione finora
- VT IndoDocumento37 pagineVT IndotyaraNessuna valutazione finora
- Atrial FlutterDocumento38 pagineAtrial FlutterLady AngodNessuna valutazione finora
- 8C - Antiarrythmic DrugsDocumento76 pagine8C - Antiarrythmic DrugsShahpoor Ahmad ShirzadaNessuna valutazione finora
- Arrhythmia: PalpitationDocumento36 pagineArrhythmia: PalpitationHala BahaaNessuna valutazione finora
- Complete Heart BlockDocumento13 pagineComplete Heart BlockSubhranil MaityNessuna valutazione finora
- Neonatal and Pediatric Guidelines Arrhythmia ManagementDocumento16 pagineNeonatal and Pediatric Guidelines Arrhythmia ManagementAkhmad HidayatNessuna valutazione finora
- TUGAS Ventricular Septal DefectDocumento8 pagineTUGAS Ventricular Septal DefectMohammad NafisNessuna valutazione finora
- Sudden Asystole During Radiofrequency Ablationa Case Report and Literature ReviewDocumento5 pagineSudden Asystole During Radiofrequency Ablationa Case Report and Literature ReviewRizkaSafitriNessuna valutazione finora
- Supraventricular TachycardiDocumento8 pagineSupraventricular TachycardiHairunisa 0049Nessuna valutazione finora
- Marathon-Related ECG ExasperationDocumento24 pagineMarathon-Related ECG ExasperationmohamedsmnNessuna valutazione finora
- ARRYHTHMIADocumento122 pagineARRYHTHMIAVimal NishadNessuna valutazione finora
- Multiprofessional Critical Care Review Course - 2005Documento16 pagineMultiprofessional Critical Care Review Course - 2005asupicuNessuna valutazione finora
- Atrial FibrillationDocumento1 paginaAtrial FibrillationshakyaNessuna valutazione finora
- What Causes Arrhythmias? What'S Its Cure: John Jero 11-DDocumento23 pagineWhat Causes Arrhythmias? What'S Its Cure: John Jero 11-DJeroNessuna valutazione finora
- Atrial FribrillationDocumento9 pagineAtrial FribrillationOwusuasare ChrispakNessuna valutazione finora
- Atrial Utter: 2 PathophysiologyDocumento4 pagineAtrial Utter: 2 PathophysiologyZiedTrikiNessuna valutazione finora
- Hypertrophic CardiomyopathyDocumento32 pagineHypertrophic CardiomyopathyAbnet WondimuNessuna valutazione finora
- C248 Focal Atrial TachycardiaDocumento3 pagineC248 Focal Atrial TachycardiaKendra KalixtaNessuna valutazione finora
- Angelina A Joho MSC in Critical Care and TraumaDocumento50 pagineAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNessuna valutazione finora
- Atrial ExtrasystoleDocumento11 pagineAtrial ExtrasystoleRaiganNessuna valutazione finora
- 1077 CMCNCHDocumento11 pagine1077 CMCNCHمحمد عقيليNessuna valutazione finora
- Wide Qrs Tachy 2Documento6 pagineWide Qrs Tachy 2Mohit TandonNessuna valutazione finora
- Acls LectureDocumento15 pagineAcls LectureVincent BautistaNessuna valutazione finora
- Penyakit Katup Jantung-Kuliah DR ErlinaDocumento70 paginePenyakit Katup Jantung-Kuliah DR ErlinaAdhiatma DotNessuna valutazione finora
- ECG InterpretationDocumento11 pagineECG InterpretationAndrea AndradaNessuna valutazione finora
- Fu 2015Documento6 pagineFu 2015redactor 1Nessuna valutazione finora
- Atrial Fibrillation: Diagnosis and TreatmentDocumento8 pagineAtrial Fibrillation: Diagnosis and TreatmentCut Thalya Alissya RahmaNessuna valutazione finora
- Wide QRS Complex Tachycardias - Causes, Epidemiology, and Clinical Manifestations - UpToDateDocumento27 pagineWide QRS Complex Tachycardias - Causes, Epidemiology, and Clinical Manifestations - UpToDateNavkiran BhartiNessuna valutazione finora
- Ventricular TachycardiaDocumento17 pagineVentricular TachycardiaAyu Rezki FadliyaNessuna valutazione finora
- Casos Cardiológicos 1Documento12 pagineCasos Cardiológicos 1Larissa SeabraNessuna valutazione finora
- 24junctional Ectopic TachycardiaDocumento3 pagine24junctional Ectopic TachycardiaZiedTrikiNessuna valutazione finora
- Bradyarrhythmiasforthe Internist: Noha Elbanhawy,, Shajil Chalil,, Khalid AbozguiaDocumento16 pagineBradyarrhythmiasforthe Internist: Noha Elbanhawy,, Shajil Chalil,, Khalid AbozguiaSantiago Ospina SanchezNessuna valutazione finora
- Transposition of Great ArteriesDocumento21 pagineTransposition of Great ArteriesAlusio Navosailagi VUNIIVI100% (1)
- Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyDocumento7 pagineBasic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest Radiographyrowd1yNessuna valutazione finora
- Supraventricular TachycardiaDocumento6 pagineSupraventricular Tachycardiaaliffikri52Nessuna valutazione finora
- Heart Valve DiseaseDocumento67 pagineHeart Valve DiseaseSaba SivaNessuna valutazione finora
- Short Cases in Medicine ColomboDocumento70 pagineShort Cases in Medicine Colombodileepa madurangaNessuna valutazione finora
- Abnomalites of ECGDocumento81 pagineAbnomalites of ECGgrreddy8364320Nessuna valutazione finora
- Ecg WorkshopDocumento39 pagineEcg WorkshopUber SnooferNessuna valutazione finora
- Valvular Heart Disease To TW FinalDocumento13 pagineValvular Heart Disease To TW FinalMohammed ElSayedNessuna valutazione finora
- Rate and RhythmDocumento10 pagineRate and RhythmSamanta Luiza de AraujoNessuna valutazione finora
- Elements and CompoundDocumento18 pagineElements and CompoundSaima Usman - 41700/TCHR/MGBNessuna valutazione finora
- Primul Meu HolterDocumento12 paginePrimul Meu Holterheraasku7194Nessuna valutazione finora
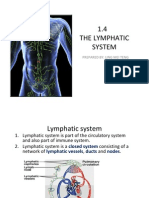
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocumento15 pagine1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingNessuna valutazione finora
- Seeley's Essentials of Anatomy & Physiology (10thDocumento4 pagineSeeley's Essentials of Anatomy & Physiology (10thZiaNessuna valutazione finora
- 14.1 The Hole Inside The Heart ABSTRAKDocumento11 pagine14.1 The Hole Inside The Heart ABSTRAKYudhistira AdiNessuna valutazione finora
- Oxford Science Fact File 3 Teaching GuideDocumento96 pagineOxford Science Fact File 3 Teaching GuideAdnan Roonjha50% (10)
- Anatomi Dan Fisiologi Sistem Kardiovaskular: Hendra FirmansyahDocumento19 pagineAnatomi Dan Fisiologi Sistem Kardiovaskular: Hendra Firmansyahrandy sepasaciNessuna valutazione finora
- The Fontan Circulation Contin EducDocumento5 pagineThe Fontan Circulation Contin EducAishu BNessuna valutazione finora
- Left-Sided Heart Failure - Symptoms, Causes and TreatmentDocumento14 pagineLeft-Sided Heart Failure - Symptoms, Causes and TreatmentHanzala Safdar AliNessuna valutazione finora
- CARDIOVASCULAR - SYSTEM Group No.3 MODULEDocumento12 pagineCARDIOVASCULAR - SYSTEM Group No.3 MODULEDavid Paul LanuzaNessuna valutazione finora
- Management of Perioperative ArrhythmiasDocumento15 pagineManagement of Perioperative Arrhythmiaszuraini_mdnoorNessuna valutazione finora
- Cardio ExamDocumento3 pagineCardio ExamImperial HinduSocNessuna valutazione finora
- A Case of Complete Heart Block With Diagnostic Challenge and Therapeutic DilemmaDocumento4 pagineA Case of Complete Heart Block With Diagnostic Challenge and Therapeutic DilemmaXo YemNessuna valutazione finora
- Heart MurmursDocumento7 pagineHeart MurmursOffvb MednuNessuna valutazione finora
- Heart Disease: Symptoms of Heart Disease in Your Blood Vessels (Atherosclerotic Disease)Documento22 pagineHeart Disease: Symptoms of Heart Disease in Your Blood Vessels (Atherosclerotic Disease)Kenneth Jay EdnacoNessuna valutazione finora
- Unit Three: The Heart: Chapter 9: Cardiac Muscle The Heart As A Pump and Function of The Heart ValvesDocumento36 pagineUnit Three: The Heart: Chapter 9: Cardiac Muscle The Heart As A Pump and Function of The Heart ValvesEbaa Moh'd ZayadnehNessuna valutazione finora
- Aj L3 CHD Qs & Ms Q1.: Diagram 1 Shows A Section Through The Heart. Diagram 1Documento9 pagineAj L3 CHD Qs & Ms Q1.: Diagram 1 Shows A Section Through The Heart. Diagram 1IntelaNessuna valutazione finora
- Frog Circulatory SystemDocumento43 pagineFrog Circulatory Systembawcock100% (5)
- Science 9 q1 Mod1 Respiratory and Circulatory System Ver FinalDocumento33 pagineScience 9 q1 Mod1 Respiratory and Circulatory System Ver Finalglam glitzNessuna valutazione finora
- Chapter 3 TRANSPORTATIONDocumento23 pagineChapter 3 TRANSPORTATIONschorynerNessuna valutazione finora
- Labe Cindy R. Worksheet 11 PDFDocumento6 pagineLabe Cindy R. Worksheet 11 PDFChristine ElnasNessuna valutazione finora
- Human Embryology:: Heart Development IIDocumento46 pagineHuman Embryology:: Heart Development IIHanifah ZainNessuna valutazione finora
- The Skeletal System WorksheetDocumento7 pagineThe Skeletal System WorksheetTavon FloydNessuna valutazione finora
- NCP Ineffective Tissue PerfusionDocumento4 pagineNCP Ineffective Tissue PerfusionSteffiNessuna valutazione finora
- 1H06B Lectures 1-4 Review CardiacDocumento16 pagine1H06B Lectures 1-4 Review Cardiachaaris 7khanNessuna valutazione finora
- Daily Lesson Log Grade 10Documento4 pagineDaily Lesson Log Grade 10Ezekiel LapitanNessuna valutazione finora
- BIOLOGYDocumento5 pagineBIOLOGYDiana NurulNessuna valutazione finora
- Summary Notes - Topic 1 Edexcel (A) Biology A LevelDocumento10 pagineSummary Notes - Topic 1 Edexcel (A) Biology A LevelAmal Abu KhalilNessuna valutazione finora
- Aortopulmonary Window in InfantsDocumento3 pagineAortopulmonary Window in Infantsonlyjust4meNessuna valutazione finora
- I Am Joe's HeartDocumento4 pagineI Am Joe's Heartbirarimahesh100% (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 4.5 su 5 stelle4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDa EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesValutazione: 4.5 su 5 stelle4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 4 su 5 stelle4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4.5 su 5 stelle4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceDa EverandTo Explain the World: The Discovery of Modern ScienceValutazione: 3.5 su 5 stelle3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDa EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsValutazione: 4.5 su 5 stelle4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlDa EverandThe Marshmallow Test: Mastering Self-ControlValutazione: 4.5 su 5 stelle4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDa EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingValutazione: 4 su 5 stelle4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (328)