Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- CPG Pcap 2012 PDFDocumento54 pagineCPG Pcap 2012 PDFroshmae67% (3)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- PrayerDocumento1 paginaPrayerHowell YapNessuna valutazione finora
- Opd Meds Jgej PDFDocumento4 pagineOpd Meds Jgej PDFKaty SanchezNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Opd Meds Jgej PDFDocumento4 pagineOpd Meds Jgej PDFKaty SanchezNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Therapeutic IndexDocumento8 pagineTherapeutic IndexHowell YapNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- For PrintingDocumento1 paginaFor PrintingHowell YapNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- W10 Water, Vitamins & MineralsDocumento37 pagineW10 Water, Vitamins & MineralsHowell YapNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- 8356Documento8 pagine8356Howell YapNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Febrile Seizure GuidelineDocumento1 paginaFebrile Seizure GuidelinesmileyginaaNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
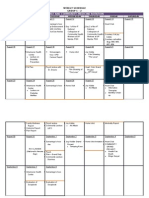
- FM Rotation Weekly Schedule Group C-2Documento2 pagineFM Rotation Weekly Schedule Group C-2Howell YapNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Compiled Case Study-LenovoDocumento24 pagineCompiled Case Study-LenovoHowell Yap100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- GitDocumento5 pagineGitHowell YapNessuna valutazione finora
- CPG Management of Dengue Infection in Adults (Revised 2nd Edition)Documento68 pagineCPG Management of Dengue Infection in Adults (Revised 2nd Edition)umiraihana1Nessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- FINAL Outcome Community Grand ProjectDocumento4 pagineFINAL Outcome Community Grand ProjectHowell YapNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- For Asthma and COPDDocumento14 pagineFor Asthma and COPDHowell YapNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Henoch SCH NleinDocumento42 pagineHenoch SCH NleinHowell YapNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Management of Febrile SeizuresDocumento13 pagineManagement of Febrile SeizuresfitriohpNessuna valutazione finora
- NDocumento1 paginaNHowell YapNessuna valutazione finora
- NDocumento6 pagineNHowell YapNessuna valutazione finora
- Lucas Vs TuanoDocumento2 pagineLucas Vs TuanoHowell YapNessuna valutazione finora
- 3b Ctc#05 Malaria 06.27.14edited2Documento28 pagine3b Ctc#05 Malaria 06.27.14edited2Howell YapNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- FCDocumento1 paginaFCHowell YapNessuna valutazione finora
- Local AnestheticsDocumento3 pagineLocal Anestheticsravi98195Nessuna valutazione finora
- DDX OsteochondromaDocumento2 pagineDDX OsteochondromaHowell YapNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- To DoDocumento1 paginaTo DoHowell YapNessuna valutazione finora
- UntitledDocumento1 paginaUntitledHowell YapNessuna valutazione finora
- Community Immersion Program FormatDocumento2 pagineCommunity Immersion Program FormatHowell YapNessuna valutazione finora
- Overview of Carbohydrates MetabolismDocumento3 pagineOverview of Carbohydrates MetabolismHowell YapNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- AnthraxDocumento3 pagineAnthraxHowell YapNessuna valutazione finora
- Doh Health ProgramsDocumento21 pagineDoh Health Programsrgng_1880304050% (2)
- Diladindafani 202162029 P8S3Documento13 pagineDiladindafani 202162029 P8S3Dila Dinda FaniNessuna valutazione finora
- Epidemiologi Prof Bhisma MurtiDocumento32 pagineEpidemiologi Prof Bhisma MurtiniaasetaNessuna valutazione finora
- Jonathan E. Narvaez: EducationDocumento1 paginaJonathan E. Narvaez: Educationapi-383581766Nessuna valutazione finora
- 28.04.2021 NTEP - RNTCP Dr. Tanuja PattankarDocumento29 pagine28.04.2021 NTEP - RNTCP Dr. Tanuja PattankarTanuja PattankarNessuna valutazione finora
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocumento1 paginaCertificate For COVID-19 Vaccination: Beneficiary DetailsNikhil shindeNessuna valutazione finora
- Neonatal Mortality, Risk Factors and Causes - A Prospective Population-Based Cohort Study in Urban PakistanDocumento7 pagineNeonatal Mortality, Risk Factors and Causes - A Prospective Population-Based Cohort Study in Urban PakistanDavid OlarinloyeNessuna valutazione finora
- MDQDocumento2 pagineMDQJavier Garcia RamosNessuna valutazione finora
- Janani Suraksha YojanaDocumento31 pagineJanani Suraksha YojanaParth PatelNessuna valutazione finora
- Hiv Case StudyDocumento2 pagineHiv Case Studyapi-485814878Nessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Philippine Guidelines On Periodic Health Examination (PHEx) PDFDocumento25 paginePhilippine Guidelines On Periodic Health Examination (PHEx) PDFLinius CruzNessuna valutazione finora
- Universal Immunization ProgrammeDocumento8 pagineUniversal Immunization ProgrammeNagaraj ReddyNessuna valutazione finora
- ID Higiene Sanitasi Pengelolaan Makanan Dan Perilaku Penjamah Makanan Di Kantin SekDocumento11 pagineID Higiene Sanitasi Pengelolaan Makanan Dan Perilaku Penjamah Makanan Di Kantin SekRini WulandariNessuna valutazione finora
- P.P.T First AidDocumento9 pagineP.P.T First AidANSHUL MEHROTTRANessuna valutazione finora
- Malawi's Newborns Report 2013Documento127 pagineMalawi's Newborns Report 2013talantasNessuna valutazione finora
- Orientation To ParentsDocumento38 pagineOrientation To ParentsHazel Ann CaspeNessuna valutazione finora
- Emerging & Re-Emerging Infections in India - An OverviewDocumento19 pagineEmerging & Re-Emerging Infections in India - An Overviewjadu777Nessuna valutazione finora
- 1 - EpidemiologyDocumento26 pagine1 - Epidemiologyhemihema75% (4)
- Immunization, Vaccines and Biologicals IVB Catalogue 2017: 13 January 2017Documento83 pagineImmunization, Vaccines and Biologicals IVB Catalogue 2017: 13 January 2017pradip_26Nessuna valutazione finora
- Peran Dan Fungsi IPCNDocumento30 paginePeran Dan Fungsi IPCNNurAnizhaNessuna valutazione finora
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocumento1 paginaCertificate For COVID-19 Vaccination: Beneficiary DetailsDDHS KANCHEEPURAMNessuna valutazione finora
- Tuskegee StudyDocumento1 paginaTuskegee Studyapi-461452779Nessuna valutazione finora
- Newer & Emerging Vaccine SynopsisDocumento13 pagineNewer & Emerging Vaccine SynopsisShikhar SinghNessuna valutazione finora
- Ebook Manfaat ASI EksklusifDocumento2 pagineEbook Manfaat ASI EksklusifwishingbabyNessuna valutazione finora
- Natural History of Disease Leavell and Clarck ModelDocumento19 pagineNatural History of Disease Leavell and Clarck ModellllloyyyyoNessuna valutazione finora
- Measures of AssociationDocumento56 pagineMeasures of AssociationAmsaluNessuna valutazione finora
- An Unquiet Mind A Memoir of Moods and Madness PDF DownloadDocumento2 pagineAn Unquiet Mind A Memoir of Moods and Madness PDF Downloadnella fornesat6% (31)
- Maternal Near MissDocumento66 pagineMaternal Near MissSafinaz InazNessuna valutazione finora
- Women Mental Health:: Postpartum DepressionDocumento62 pagineWomen Mental Health:: Postpartum DepressionTickablingbling Alwaysshine Likeatenglarious100% (1)
- Hippocrates - The Father of MedicineDocumento1 paginaHippocrates - The Father of Medicine123121Nessuna valutazione finora
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (24)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4 su 5 stelle4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (80)