Potrebbero piacerti anche
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Crp-DikonversiDocumento13 pagineCrp-DikonversiKurnia FitriasariNessuna valutazione finora
- Problem-based Approach to Gastroenterology and HepatologyDa EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNessuna valutazione finora
- Serum ElectrolytesDocumento2 pagineSerum ElectrolytesKervin CablaidaNessuna valutazione finora
- Hemoglobin and HematocritDocumento9 pagineHemoglobin and HematocritLovely B. AlipatNessuna valutazione finora
- Case Study 2Documento4 pagineCase Study 2api-2451636590% (1)
- Ascitic Fluid AnalysisDocumento3 pagineAscitic Fluid AnalysisLohJNessuna valutazione finora
- Management of Tuberculosis: A guide for clinicians (eBook edition)Da EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Nessuna valutazione finora
- Thalassemia Case StudyDocumento13 pagineThalassemia Case StudyNellyWataNessuna valutazione finora
- Infective Endocarditis: A Multidisciplinary ApproachDa EverandInfective Endocarditis: A Multidisciplinary ApproachArman KilicNessuna valutazione finora
- UrinalysisDocumento32 pagineUrinalysiskholoud220Nessuna valutazione finora
- Renal Stones A Clinical Review PDFDocumento6 pagineRenal Stones A Clinical Review PDFNurholis MajidNessuna valutazione finora
- AtaxiaDocumento8 pagineAtaxiaDivya Gupta0% (1)
- Anemia IntroductionDocumento15 pagineAnemia IntroductionNitesh Kotian100% (1)
- Rhabdomyolysis Case Study WeeblyDocumento18 pagineRhabdomyolysis Case Study Weeblyapi-241865788Nessuna valutazione finora
- Addison's DiseaseDocumento9 pagineAddison's Diseaseash ashNessuna valutazione finora
- Nephrotic Syndrome (Nephrosis)Documento9 pagineNephrotic Syndrome (Nephrosis)Radit Radovzky MayangkaraNessuna valutazione finora
- HaemoglobinDocumento47 pagineHaemoglobinPreethi AbhilashNessuna valutazione finora
- Routine UrinalysisDocumento4 pagineRoutine UrinalysisDanica Joy Christelle L. PilarNessuna valutazione finora
- Elisa & RiaDocumento4 pagineElisa & Riadihajum3Nessuna valutazione finora
- Fibrinogen - CLAUSSDocumento1 paginaFibrinogen - CLAUSSfurqaan_610Nessuna valutazione finora
- Analysis of UrineDocumento5 pagineAnalysis of UrineHaridha ChandranNessuna valutazione finora
- Vii. Laboratory Results: Hemoglobin 129 MG/DL 140-160 MG/DL LowDocumento2 pagineVii. Laboratory Results: Hemoglobin 129 MG/DL 140-160 MG/DL LowAdrian Dela CruzNessuna valutazione finora
- Classification of AnemiaDocumento33 pagineClassification of Anemialieynna4996Nessuna valutazione finora
- (Osborn) Chapter 51: Learning Outcomes (Number and Title)Documento16 pagine(Osborn) Chapter 51: Learning Outcomes (Number and Title)KittiesNessuna valutazione finora
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocumento44 paginePractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarNessuna valutazione finora
- UrinalysisDocumento9 pagineUrinalysisSukma EffendyNessuna valutazione finora
- Bleeding Case SampleDocumento7 pagineBleeding Case SampleNikko CabrestanteNessuna valutazione finora
- Venous Thromboembolism (VTE) - McMaster Pathophysiology ReviewDocumento9 pagineVenous Thromboembolism (VTE) - McMaster Pathophysiology ReviewFadiyah UlfahNessuna valutazione finora
- Hemorrhagic Cerebro Vascular DiseaseDocumento37 pagineHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Beta LactamDocumento18 pagineBeta LactamCesar Saba0% (1)
- Diabetes NotesDocumento10 pagineDiabetes Notestripj33Nessuna valutazione finora
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingDa EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNessuna valutazione finora
- Massive Blood TransfusionDocumento17 pagineMassive Blood TransfusionevanNessuna valutazione finora
- Blood Group Systems ISBTDocumento25 pagineBlood Group Systems ISBTkusumahpratiwi100% (1)
- Case Study On AsthmaDocumento3 pagineCase Study On AsthmaNurudeen Ibrahim100% (1)
- Genpath 04 - RENAL LABORATORY TESTS - ppt.MEd 2016 (Ninaarajade's Conflicted Copy 2016-10-29) (ASUS's Conflicted Copy 2016-11-14)Documento67 pagineGenpath 04 - RENAL LABORATORY TESTS - ppt.MEd 2016 (Ninaarajade's Conflicted Copy 2016-10-29) (ASUS's Conflicted Copy 2016-11-14)RjDNessuna valutazione finora
- Therapeutic Drug MonitoringDocumento8 pagineTherapeutic Drug MonitoringLourdette TorrefielNessuna valutazione finora
- Renal DisordersDocumento77 pagineRenal Disorderslorelee_espaldon100% (1)
- Diabetes InsipidusDocumento60 pagineDiabetes Insipidusperie_md100% (1)
- Anatomy & PhysiologyDocumento9 pagineAnatomy & Physiologyrachael80% (5)
- Unit Kajian Dan Maklumat Drug (Ukmd), Husm. Adr Case ReportDocumento56 pagineUnit Kajian Dan Maklumat Drug (Ukmd), Husm. Adr Case ReportRendry Dwitya WirawanNessuna valutazione finora
- Hypokalemia 180813073624Documento26 pagineHypokalemia 180813073624korotkofNessuna valutazione finora
- Potassium DeterminationDocumento1 paginaPotassium DeterminationEl Marie SalungaNessuna valutazione finora
- Case 2 and 3 Q1Documento3 pagineCase 2 and 3 Q1Jeffrey Ramos0% (1)
- HYPERAMMONEMIADocumento10 pagineHYPERAMMONEMIANaisha JNessuna valutazione finora
- Manchester Anaemia GuideDocumento13 pagineManchester Anaemia Guidemubzy14Nessuna valutazione finora
- Asthma in the 21st Century: New Research AdvancesDa EverandAsthma in the 21st Century: New Research AdvancesRachel NadifNessuna valutazione finora
- Complement SystemDocumento6 pagineComplement SystemJimit GandhiNessuna valutazione finora
- Bone Marrow TransplantationDocumento21 pagineBone Marrow TransplantationMorrison George100% (1)
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocumento43 paginePamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNessuna valutazione finora
- New Concepts in the Management of Septic Perianal ConditionsDa EverandNew Concepts in the Management of Septic Perianal ConditionsNessuna valutazione finora
- Diagnosis of Gastrointestinal Bleeding in AdultsDocumento8 pagineDiagnosis of Gastrointestinal Bleeding in AdultsSaeed Al-YafeiNessuna valutazione finora
- PSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionDocumento7 paginePSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionMichael TobilobaNessuna valutazione finora
- Lecture 28 - Pathology of DiabetesDocumento34 pagineLecture 28 - Pathology of Diabetesapi-3703352100% (4)
- What Is The Oral Glucose Tolerance TestDocumento2 pagineWhat Is The Oral Glucose Tolerance TestBianca Camille100% (1)
- Hodgkin's DiseaseDocumento58 pagineHodgkin's Diseasealibayaty1Nessuna valutazione finora
- PresentationDocumento6 paginePresentationVruchali ThakareNessuna valutazione finora
- COE301 Lab 2 Introduction MIPS AssemblyDocumento7 pagineCOE301 Lab 2 Introduction MIPS AssemblyItz Sami UddinNessuna valutazione finora
- The Impact of Online Games To The AcademicDocumento20 pagineThe Impact of Online Games To The AcademicJessica BacaniNessuna valutazione finora
- Recent Advances in Dielectric-Resonator Antenna TechnologyDocumento14 pagineRecent Advances in Dielectric-Resonator Antenna Technologymarceloassilva7992Nessuna valutazione finora
- An Overview of Marketing - Week 1Documento7 pagineAn Overview of Marketing - Week 1Jowjie TVNessuna valutazione finora
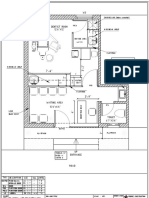
- Dental Clinic - Floor Plan R3-2Documento1 paginaDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- Permeability PropertiesDocumento12 paginePermeability Propertieskiwi27_87Nessuna valutazione finora
- Physical Characteristics of SoilDocumento26 paginePhysical Characteristics of SoillfpachecoNessuna valutazione finora
- A Guide To Funeral Ceremonies and PrayersDocumento26 pagineA Guide To Funeral Ceremonies and PrayersJohn DoeNessuna valutazione finora
- Datasheet Brahma (2023)Documento8 pagineDatasheet Brahma (2023)Edi ForexNessuna valutazione finora
- Statistics and Probability Course Syllabus (2023) - SignedDocumento3 pagineStatistics and Probability Course Syllabus (2023) - SignedDarence Fujihoshi De AngelNessuna valutazione finora
- Hypoglycemia After Gastric Bypass Surgery. Current Concepts and Controversies 2018Documento12 pagineHypoglycemia After Gastric Bypass Surgery. Current Concepts and Controversies 2018Rio RomaNessuna valutazione finora
- Aa DistriDocumento3 pagineAa Distriakosiminda143Nessuna valutazione finora
- Fortigate System Admin 40 Mr2Documento115 pagineFortigate System Admin 40 Mr2KhaleelNessuna valutazione finora
- The 100 Best Books For 1 Year Olds: Board Book HardcoverDocumento17 pagineThe 100 Best Books For 1 Year Olds: Board Book Hardcovernellie_74023951Nessuna valutazione finora
- EN 213 Vertintojui WWWDocumento2 pagineEN 213 Vertintojui WWWMonika PetronytėNessuna valutazione finora
- Hamza Akbar: 0308-8616996 House No#531A-5 O/S Dehli Gate MultanDocumento3 pagineHamza Akbar: 0308-8616996 House No#531A-5 O/S Dehli Gate MultanTalalNessuna valutazione finora
- ZEROPAY WhitepaperDocumento15 pagineZEROPAY WhitepaperIlham NurrohimNessuna valutazione finora
- ShotcreteDocumento7 pagineShotcreteafuhcivNessuna valutazione finora
- Operaciones UnitariasDocumento91 pagineOperaciones UnitariasAlejandro ReyesNessuna valutazione finora
- Crop Science SyllabusDocumento42 pagineCrop Science Syllabusbetty makushaNessuna valutazione finora
- TDS-11SH Top Drive D392004689-MKT-001 Rev. 01Documento2 pagineTDS-11SH Top Drive D392004689-MKT-001 Rev. 01Israel Medina100% (2)
- Benefits and Drawbacks of Thermal Pre-Hydrolysis For Operational Performance of Wastewater Treatment PlantsDocumento7 pagineBenefits and Drawbacks of Thermal Pre-Hydrolysis For Operational Performance of Wastewater Treatment PlantsmartafhNessuna valutazione finora
- Myth or Fact-Worksheet 1Documento1 paginaMyth or Fact-Worksheet 1Zahraa LotfyNessuna valutazione finora
- LUNG ARTIFACTSreviewDocumento13 pagineLUNG ARTIFACTSreviewMayra ValderramaNessuna valutazione finora
- Green ChemistryDocumento17 pagineGreen ChemistryAaditya RamanNessuna valutazione finora
- Prevention of Power Theft Using Concept of Multifunction Meter and PLCDocumento6 paginePrevention of Power Theft Using Concept of Multifunction Meter and PLCMuhammad FarhanNessuna valutazione finora
- The Politics of GenreDocumento21 pagineThe Politics of GenreArunabha ChaudhuriNessuna valutazione finora
- Bridging The Divide Between Saas and Enterprise Datacenters: An Oracle White Paper Feb 2010Documento18 pagineBridging The Divide Between Saas and Enterprise Datacenters: An Oracle White Paper Feb 2010Danno NNessuna valutazione finora
- The Hot Aishwarya Rai Wedding and Her Life.20130105.040216Documento2 pagineThe Hot Aishwarya Rai Wedding and Her Life.20130105.040216anon_501746111100% (1)