Potrebbero piacerti anche
- Missouri Affidavit For Head of Family Exemption of Wages GarnishmentDocumento2 pagineMissouri Affidavit For Head of Family Exemption of Wages GarnishmentitargetingNessuna valutazione finora
- Missouri General Affidavit FormDocumento1 paginaMissouri General Affidavit FormitargetingNessuna valutazione finora
- Missouri Child Custody FormDocumento46 pagineMissouri Child Custody Formitargeting0% (1)
- Missouri Bill of SaleDocumento1 paginaMissouri Bill of SaleitargetingNessuna valutazione finora
- Bank Statement 4Documento4 pagineBank Statement 4Jardan Nelli86% (7)
- Missouri Form Mo W 4Documento1 paginaMissouri Form Mo W 4itargetingNessuna valutazione finora
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Da EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Valutazione: 1 su 5 stelle1/5 (1)
- TD Bank StatementDocumento3 pagineTD Bank StatementdeepdokNessuna valutazione finora
- How To File Your Own Bankruptcy: The Step-by-Step Handbook to Filing Your Own Bankruptcy PetitionDa EverandHow To File Your Own Bankruptcy: The Step-by-Step Handbook to Filing Your Own Bankruptcy PetitionNessuna valutazione finora
- The Nigerian Society of EngineersDocumento14 pagineThe Nigerian Society of EngineersemmanuelNessuna valutazione finora
- Missouri Separation Agreement TemplateDocumento66 pagineMissouri Separation Agreement TemplateitargetingNessuna valutazione finora
- Missouri Separation Agreement TemplateDocumento66 pagineMissouri Separation Agreement TemplateitargetingNessuna valutazione finora
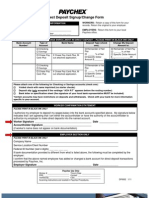
- Direct Deposit FormDocumento3 pagineDirect Deposit FormRabindra ShakyaNessuna valutazione finora
- 1199 A 1 PDFDocumento4 pagine1199 A 1 PDFGerry Ruff100% (1)
- 8.31.21 Boa STMNTDocumento6 pagine8.31.21 Boa STMNTAnthony VinsonNessuna valutazione finora
- Missouri Offer To Purchase Real Estate FormDocumento5 pagineMissouri Offer To Purchase Real Estate FormitargetingNessuna valutazione finora
- Sf1199a 870601V01Documento2 pagineSf1199a 870601V01jefe_e578726Nessuna valutazione finora
- Bank Authorization (BA) FormDocumento4 pagineBank Authorization (BA) FormAilec FinancesNessuna valutazione finora
- Care Credit AppDocumento7 pagineCare Credit AppwvhvetNessuna valutazione finora
- Bcbs - HCSC IllinoisDocumento2 pagineBcbs - HCSC IllinoisShirley Pigott MDNessuna valutazione finora
- SynchronyDocumento11 pagineSynchronytestrun555100% (1)
- Security Bank Personal Loan App FormDocumento2 pagineSecurity Bank Personal Loan App FormDemp Almiranez75% (4)
- Missouri Last Will and Testament FormDocumento7 pagineMissouri Last Will and Testament Formitargeting100% (1)
- Missouri Quitclaim Deed Form 1Documento2 pagineMissouri Quitclaim Deed Form 1itargetingNessuna valutazione finora
- Direct Deposit FormDocumento3 pagineDirect Deposit FormSreenivas RaoNessuna valutazione finora
- Account Opening Form and Investment FormDocumento5 pagineAccount Opening Form and Investment FormEngr Muhammad Talha IslamNessuna valutazione finora
- CitiBank ApplicationDocumento15 pagineCitiBank ApplicationJordan P HunterNessuna valutazione finora
- Life Insurance and Its Mathematical BasisDocumento374 pagineLife Insurance and Its Mathematical BasisAvinash Veerendra TakNessuna valutazione finora
- Roman Catholic Bishop of Jaro V. de La Pena 26 Phil 144 (Aquino) FactsDocumento8 pagineRoman Catholic Bishop of Jaro V. de La Pena 26 Phil 144 (Aquino) FactsChin MartinzNessuna valutazione finora
- Direct Deposit FormDocumento2 pagineDirect Deposit FormCamiloNessuna valutazione finora
- CFPB Sample Notice of Unauthorized TransferDocumento2 pagineCFPB Sample Notice of Unauthorized Transferinfo amlakNessuna valutazione finora
- Credit Repair Plan B Expedite Agreement 05-13-16Documento9 pagineCredit Repair Plan B Expedite Agreement 05-13-16Plan B CRSNessuna valutazione finora
- Electronic Deposit Instructions DIRECT DEPOSITDocumento4 pagineElectronic Deposit Instructions DIRECT DEPOSITPedro PerezNessuna valutazione finora
- Company Check EPayDocumento7 pagineCompany Check EPayWes SwensonNessuna valutazione finora
- TSYS Bank Request Change Document-101Documento1 paginaTSYS Bank Request Change Document-101Keller Brown JnrNessuna valutazione finora
- Account Statement 011219 290220Documento14 pagineAccount Statement 011219 290220ManishNessuna valutazione finora
- Bank Switching Step by Step N Standard Forms Made EasyDocumento6 pagineBank Switching Step by Step N Standard Forms Made EasyBenjamin LinuseNessuna valutazione finora
- Account StatementDocumento3 pagineAccount StatementJobz ForuNessuna valutazione finora
- Withdrawal of Contributions AppDocumento7 pagineWithdrawal of Contributions AppJoey Daniel FinleyNessuna valutazione finora
- Direct Deposit FormDocumento1 paginaDirect Deposit FormLatonya DodsonNessuna valutazione finora
- Islamic Financial System and Conventional Banking: A ComparisonDocumento13 pagineIslamic Financial System and Conventional Banking: A ComparisonDenis IoniţăNessuna valutazione finora
- Final Internship Report On Summit Bank by Ibrar A. QaziDocumento50 pagineFinal Internship Report On Summit Bank by Ibrar A. QaziAbrar Ahmed Qazi82% (11)
- Punjab State Cooperative BankDocumento58 paginePunjab State Cooperative BankRavneet Singh75% (4)
- Secondary Direct DepositDocumento1 paginaSecondary Direct DepositParamintaramaha ParamintaramahaNessuna valutazione finora
- Abd Direct Deposit InfoDocumento2 pagineAbd Direct Deposit Infobrysonblair23Nessuna valutazione finora
- Uib 1091aDocumento2 pagineUib 1091aJoseph SantosNessuna valutazione finora
- Ag 501Documento2 pagineAg 501Cindy FazzinoNessuna valutazione finora
- Truist Ach FormDocumento1 paginaTruist Ach FormhugstinsNessuna valutazione finora
- BSP Application FormDocumento2 pagineBSP Application FormTyphonNessuna valutazione finora
- Membership Update FormDocumento4 pagineMembership Update FormbmapiraNessuna valutazione finora
- In-Service Withdrawal FormDocumento1 paginaIn-Service Withdrawal FormlanzahouseNessuna valutazione finora
- Cigna Claim FormDocumento2 pagineCigna Claim FormLoganBohannonNessuna valutazione finora
- SSSFormDocumento2 pagineSSSFormCY Lee100% (1)
- Meaning of National AnthemDocumento1 paginaMeaning of National Anthemmanishchaudhry73Nessuna valutazione finora
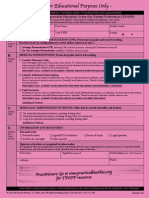
- Application For Refund of Educational Contributions: (VEAP, Chapter 32, Title 38, U.S.C.)Documento2 pagineApplication For Refund of Educational Contributions: (VEAP, Chapter 32, Title 38, U.S.C.)Emette E. MasseyNessuna valutazione finora
- Canada EngDocumento3 pagineCanada Engpaolomarabella8Nessuna valutazione finora
- Inbound 8444811727727021917Documento10 pagineInbound 8444811727727021917RishiNessuna valutazione finora
- 197 - Excess Contribution and Deposit Correcti..Documento1 pagina197 - Excess Contribution and Deposit Correcti..tdrkNessuna valutazione finora
- 2016 SSS Loan Form PDFDocumento4 pagine2016 SSS Loan Form PDFAnonymous 1AXVu3Gh60% (5)
- Update of Payment Method Letter FinalDocumento2 pagineUpdate of Payment Method Letter Finaljiarou0313Nessuna valutazione finora
- EPCORPaymentPlanApplication EdmontonFortisDocumento3 pagineEPCORPaymentPlanApplication EdmontonFortiskevinatstarburstNessuna valutazione finora
- SwitchKit ExampleDocumento7 pagineSwitchKit ExamplefindabetterbankNessuna valutazione finora
- PL FormDocumento2 paginePL FormRonald TemajoNessuna valutazione finora
- Direct Debit Request FormDocumento2 pagineDirect Debit Request FormrenjerNessuna valutazione finora
- Customer Information Sheet: Primary Account HolderDocumento7 pagineCustomer Information Sheet: Primary Account HolderJayakumarNessuna valutazione finora
- Calamity HMDFDocumento3 pagineCalamity HMDFchennieNessuna valutazione finora
- BUCKS CONCRETE & PAVERS INC - AmTrust Workers' Compensation PolicyDocumento37 pagineBUCKS CONCRETE & PAVERS INC - AmTrust Workers' Compensation PolicyYvette BroadwaterNessuna valutazione finora
- Direct Deposit of Other Income: Please Establish Direct Deposit or Change Account Used For Direct DepositDocumento1 paginaDirect Deposit of Other Income: Please Establish Direct Deposit or Change Account Used For Direct DepositXquisiteNessuna valutazione finora
- How To Request Direct DepositDocumento1 paginaHow To Request Direct DepositalithebigbossNessuna valutazione finora
- Bills2Pay AppForm 2012Documento1 paginaBills2Pay AppForm 2012Anonymous ku7POqvKNessuna valutazione finora
- SLF002 CalamityLoanApplication V05-2Documento2 pagineSLF002 CalamityLoanApplication V05-2LouiseNessuna valutazione finora
- Dir DepDocumento1 paginaDir Depfazlah8106Nessuna valutazione finora
- UnknownDocumento17 pagineUnknownEnglcom-Barrot PublisherNessuna valutazione finora
- University National Bank ("Bank") Refund Transfer Application and AgreementDocumento6 pagineUniversity National Bank ("Bank") Refund Transfer Application and AgreementMètrès Rosie-Rose AimableNessuna valutazione finora
- Please Complete and Return This Form With A Void Cheque To Customer Care Centre by Mail, Fax or EmailDocumento1 paginaPlease Complete and Return This Form With A Void Cheque To Customer Care Centre by Mail, Fax or EmailAmirhoosein MeshginiNessuna valutazione finora
- The Most Effective Credit Bureau Dispute LetterDocumento16 pagineThe Most Effective Credit Bureau Dispute LettercjNessuna valutazione finora
- Calamity Loan Application Form (CLAF, HQP-SLF-066) (Applicable To Imus Branch Members Only)Documento2 pagineCalamity Loan Application Form (CLAF, HQP-SLF-066) (Applicable To Imus Branch Members Only)egabad78% (9)
- Lincoln Withdrawal AgreementDocumento2 pagineLincoln Withdrawal Agreementmaraure2013Nessuna valutazione finora
- Debt Reduction Without DefaultDocumento13 pagineDebt Reduction Without DefaultitargetingNessuna valutazione finora
- Missouri Emergency Medical Release FormDocumento1 paginaMissouri Emergency Medical Release FormitargetingNessuna valutazione finora
- Missouri Do Not Resuscitate FormDocumento1 paginaMissouri Do Not Resuscitate Formitargeting0% (1)
- Missouri Liability Release and Waiver FormDocumento2 pagineMissouri Liability Release and Waiver FormitargetingNessuna valutazione finora
- Missouri Medical Record Release Form 1Documento1 paginaMissouri Medical Record Release Form 1itargetingNessuna valutazione finora
- Missouri Report Your Workplace Injury or Occupational Disease or Repetitive Trauma InjuryDocumento1 paginaMissouri Report Your Workplace Injury or Occupational Disease or Repetitive Trauma InjuryitargetingNessuna valutazione finora
- Missouri Transportable Physician Orders For Patient Preferences Tpopp FormDocumento2 pagineMissouri Transportable Physician Orders For Patient Preferences Tpopp FormitargetingNessuna valutazione finora
- Tut 3 Group 15 Vietcombank ReportDocumento22 pagineTut 3 Group 15 Vietcombank ReportNgọc LinhNessuna valutazione finora
- Internship Report On Deposit of Shahjalal Islami Bank LTDDocumento50 pagineInternship Report On Deposit of Shahjalal Islami Bank LTDChowdhury Mahin Ahmed0% (1)
- Company Profile BoiDocumento29 pagineCompany Profile BoiPrince Satish ReddyNessuna valutazione finora
- BAFDocumento100 pagineBAFiftikharhayderNessuna valutazione finora
- BSA2A WrittenReports Thrift-BanksDocumento5 pagineBSA2A WrittenReports Thrift-Banksrobert pilapilNessuna valutazione finora
- Wollega University Shambu Campus: Advisor: Adugna (MSC)Documento38 pagineWollega University Shambu Campus: Advisor: Adugna (MSC)Adugna Megenasa100% (1)
- Internship-Report-on-General-Banking-of-Janata-Bank-Limited 2Documento35 pagineInternship-Report-on-General-Banking-of-Janata-Bank-Limited 2Bronson CastroNessuna valutazione finora
- Commercial Banking in IndiaDocumento11 pagineCommercial Banking in IndiaTony SharmaNessuna valutazione finora
- InsuranceDocumento188 pagineInsurancetura kedirNessuna valutazione finora
- Risk Exposure and Risk Management at Korea First Bank 2023Documento24 pagineRisk Exposure and Risk Management at Korea First Bank 2023Mariola TiradorNessuna valutazione finora
- Submitted By-Prabhakar Rahul PGDM 2009 - 2011 Enrollment No - 2009PGDM031Documento76 pagineSubmitted By-Prabhakar Rahul PGDM 2009 - 2011 Enrollment No - 2009PGDM031Prabhakar RahulNessuna valutazione finora
- Handbook On AIS Icome TaxDocumento102 pagineHandbook On AIS Icome TaxArun Kumar NathaNessuna valutazione finora
- Internship ReportDocumento43 pagineInternship ReportAunto P PonnachanNessuna valutazione finora
- HKALE Money and BankingDocumento5 pagineHKALE Money and BankingAngela SinNessuna valutazione finora
- Account Statement: Penyata AkaunDocumento8 pagineAccount Statement: Penyata Akaunsgconstruction94Nessuna valutazione finora
- Bank of Kigali Announces Q1 2010 ResultsDocumento7 pagineBank of Kigali Announces Q1 2010 ResultsBank of KigaliNessuna valutazione finora
- 4 Preparing A Bank ReconciliationDocumento9 pagine4 Preparing A Bank ReconciliationSamuel DebebeNessuna valutazione finora
- Express AccountOpeningDocumento7 pagineExpress AccountOpeningSheraz AbbasNessuna valutazione finora
- CashDocumento16 pagineCashJemson YandugNessuna valutazione finora
- Compre FAR19Documento16 pagineCompre FAR19Gwen Cabarse PansoyNessuna valutazione finora
- Chapter 4Documento39 pagineChapter 4Pratikshya KarkiNessuna valutazione finora