Potrebbero piacerti anche
- How to Maximize the Caloric Costs of Exercise: A Relatively Short StoryDa EverandHow to Maximize the Caloric Costs of Exercise: A Relatively Short StoryNessuna valutazione finora
- Energy Balance Body Composition & Weight ManagementDocumento38 pagineEnergy Balance Body Composition & Weight ManagementMozil Fadzil KamarudinNessuna valutazione finora
- Praktikum-Perhitungan Kebutuhan NutrisiDocumento34 paginePraktikum-Perhitungan Kebutuhan NutrisivandelNessuna valutazione finora
- Lab 6 (Energy Balance)Documento3 pagineLab 6 (Energy Balance)Kelvin FookNessuna valutazione finora
- Anthropometrics and Assessment of Energy ExpenditureDocumento40 pagineAnthropometrics and Assessment of Energy ExpenditureJennifer AnguloNessuna valutazione finora
- Nutrition ENERGYDocumento37 pagineNutrition ENERGYMael LehsNessuna valutazione finora
- Energyexpenditure 160422165403 PDFDocumento15 pagineEnergyexpenditure 160422165403 PDFmehdi.chlif4374Nessuna valutazione finora
- Caloric BalanceDocumento16 pagineCaloric Balanceआशिष दादाNessuna valutazione finora
- Energy Value of FoodsDocumento72 pagineEnergy Value of FoodsKen Ryan DizonNessuna valutazione finora
- Dietary ComputationDocumento17 pagineDietary ComputationFlas Floresta0% (1)
- Physiologic Value of FoodDocumento46 paginePhysiologic Value of FoodMICHELLE FACTONessuna valutazione finora
- Swami Shraddhanand CollegeDocumento25 pagineSwami Shraddhanand CollegegunjanNessuna valutazione finora
- 9 Physiologic Value of FoodDocumento40 pagine9 Physiologic Value of FoodJason LumayaNessuna valutazione finora
- Body Composition and Weight Management Lecture 2022Documento64 pagineBody Composition and Weight Management Lecture 2022Eiva QuinnNessuna valutazione finora
- AnthropometryDocumento48 pagineAnthropometryRisma Anjelina0% (1)
- BMR CalculatorDocumento1 paginaBMR Calculatorchris45syccNessuna valutazione finora
- Nutrition & Diet Therapy: By: Odessa S. Bugarin, ManDocumento46 pagineNutrition & Diet Therapy: By: Odessa S. Bugarin, ManWincy SalazarNessuna valutazione finora
- Impact of Exercise and Diet On Resting Metabolic Rate: by Sonali Tushamer MPT Semester 1Documento16 pagineImpact of Exercise and Diet On Resting Metabolic Rate: by Sonali Tushamer MPT Semester 1sonali tushamer100% (1)
- Weight ManagementDocumento32 pagineWeight ManagementRoisinNessuna valutazione finora
- Tuesday Nutrition 21-3-23.Documento75 pagineTuesday Nutrition 21-3-23.Sanjeev walvekarNessuna valutazione finora
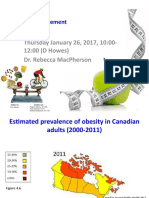
- Thursday January 26, 2017, 10:00-12:00 (D Howes) Dr. Rebecca MacphersonDocumento19 pagineThursday January 26, 2017, 10:00-12:00 (D Howes) Dr. Rebecca MacphersonpaigeNessuna valutazione finora
- BMR CalculatorDocumento4 pagineBMR Calculatorharshika tembhurneNessuna valutazione finora
- Screenshot 2024-01-13 at 14.51.57Documento1 paginaScreenshot 2024-01-13 at 14.51.57angelasaguirre573Nessuna valutazione finora
- ObesityDocumento91 pagineObesityAnkit Raj MehtaNessuna valutazione finora
- Metabolism and NutritionDocumento69 pagineMetabolism and NutritionNur Nadrah Hasfinie HasanuddinNessuna valutazione finora
- BMR CalculatorDocumento1 paginaBMR Calculatorfoxxxpuppie2Nessuna valutazione finora
- Component of Energy ExpenditureDocumento14 pagineComponent of Energy ExpenditureAnahgen RomeoNessuna valutazione finora
- Energy Intake and ExpenditureDocumento38 pagineEnergy Intake and ExpenditureNichNessuna valutazione finora
- Energy Metabolism 3Documento41 pagineEnergy Metabolism 3Anam FatimaNessuna valutazione finora
- Energy NeedsDocumento5 pagineEnergy NeedsValieiev ArtemNessuna valutazione finora
- 1 Lecture-in-LaboratoryDocumento6 pagine1 Lecture-in-LaboratoryTrinidad SherwinNessuna valutazione finora
- Engineering A Healthy Body: Career CatalystDocumento6 pagineEngineering A Healthy Body: Career CatalystB6D4N0Nessuna valutazione finora
- Human Energy Expenditure During Rest and Physical ActivityDocumento46 pagineHuman Energy Expenditure During Rest and Physical ActivityKamyab Sadeghzadeh100% (2)
- Energy Balance and Weight Maintenance: Ghina Assaf Chedid, Msc. Fundamentals of Human NutritionDocumento48 pagineEnergy Balance and Weight Maintenance: Ghina Assaf Chedid, Msc. Fundamentals of Human NutritionYouness Abou SalehNessuna valutazione finora
- School of Arts & Sciences Natural Science Department: PED 291 - Physical Fitness Final Exam - Spring 2017Documento12 pagineSchool of Arts & Sciences Natural Science Department: PED 291 - Physical Fitness Final Exam - Spring 2017Eliot KhNessuna valutazione finora
- 1-Energy Balance and Control of Body WeightDocumento42 pagine1-Energy Balance and Control of Body Weightybalepa9Nessuna valutazione finora
- Dietary ComputationsDocumento33 pagineDietary ComputationsVincent Maralit MaterialNessuna valutazione finora
- Energy Expenditure LabDocumento6 pagineEnergy Expenditure Labapi-311106200Nessuna valutazione finora
- Body WeightDocumento26 pagineBody WeightJOMAR ASPIRASNessuna valutazione finora
- Metabolism 1 1819Documento28 pagineMetabolism 1 1819Liaqat HussainNessuna valutazione finora
- Basal Metabollic Rate (BMR)Documento16 pagineBasal Metabollic Rate (BMR)ibnu affanNessuna valutazione finora
- Class Note NUT 301 - 3 - ENERGY REQUIREMENTSDocumento13 pagineClass Note NUT 301 - 3 - ENERGY REQUIREMENTSomonzejele jenniferNessuna valutazione finora
- Untitled 1 OpenDocumento3 pagineUntitled 1 OpenTom JonesNessuna valutazione finora
- Energy Balance and Weight Control: Reed A Berger MD Visiting Clinical Professor NutritionDocumento29 pagineEnergy Balance and Weight Control: Reed A Berger MD Visiting Clinical Professor NutritionMuthiaranifsNessuna valutazione finora
- Energy Balance 2021Documento43 pagineEnergy Balance 2021Jessica SnowNessuna valutazione finora
- ON Education Module 3Documento33 pagineON Education Module 3Sajedur RahmanNessuna valutazione finora
- 13 - Lecture #8 - Energy BalanceDocumento56 pagine13 - Lecture #8 - Energy Balancekram aquinoNessuna valutazione finora
- Nutririon Sec1 NEW FinalDocumento40 pagineNutririon Sec1 NEW FinalMOSTAFA HAMDYNessuna valutazione finora
- February MathoffitnessDocumento25 pagineFebruary Mathoffitnessfitnesadvice11 blogspot comNessuna valutazione finora
- Calculating Diets and Meal PlanningDocumento26 pagineCalculating Diets and Meal Planningjezreel ibarra100% (2)
- Lecture 3 NewDocumento40 pagineLecture 3 Newselin safranNessuna valutazione finora
- Nutrition Folio (Basal Metabolic Rate)Documento15 pagineNutrition Folio (Basal Metabolic Rate)Nursakinah NajwahNessuna valutazione finora
- CalculateCalorie Needs and Macronutrients - Bodybuilding - Com ForumsDocumento3 pagineCalculateCalorie Needs and Macronutrients - Bodybuilding - Com ForumsTyler DavisNessuna valutazione finora
- Group 6 Energy ExpenditureDocumento24 pagineGroup 6 Energy ExpenditureellehcordochelleNessuna valutazione finora
- Measurement of Body CompositionDocumento7 pagineMeasurement of Body CompositionNeha Dubey100% (3)
- EER WorksheetDocumento3 pagineEER WorksheetMichael PoddubnyNessuna valutazione finora
- Knab 2011Documento24 pagineKnab 2011Johanna Maria HänggiNessuna valutazione finora
- Nutrition Guideline For Neuro-Psychiatry Practice: Nurpudji A.Taslim Andi FaradilahDocumento32 pagineNutrition Guideline For Neuro-Psychiatry Practice: Nurpudji A.Taslim Andi FaradilahAnonymous brP4W9YNessuna valutazione finora
- Metabolic Stress II (Burn) 2020Documento37 pagineMetabolic Stress II (Burn) 2020ﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞNessuna valutazione finora
- Path Phys3Documento73 paginePath Phys3Наталія Вікторівна ДавиденкоNessuna valutazione finora
- Nutrition and Feed TechnologyDocumento29 pagineNutrition and Feed TechnologyAmitabh ChoudhuryNessuna valutazione finora
- Inborn Errors of CHO MetabolismDocumento30 pagineInborn Errors of CHO Metabolismwaleedemad649Nessuna valutazione finora
- 5.0 Hormonal Control of Carbohydrate MetabolismDocumento10 pagine5.0 Hormonal Control of Carbohydrate Metabolismeka saputraNessuna valutazione finora
- Carbohydrate MetabolismDocumento43 pagineCarbohydrate MetabolismMarliza CauntaoNessuna valutazione finora
- Pharm-D 011014 PDFDocumento106 paginePharm-D 011014 PDFSeethalakshmiNessuna valutazione finora
- Nutrition For Sport and Exercise Mindtap Course List 5Th Edition Marie Dunford Full ChapterDocumento67 pagineNutrition For Sport and Exercise Mindtap Course List 5Th Edition Marie Dunford Full Chaptercharles.martinez668Nessuna valutazione finora
- Nutrition and MetabolismDocumento179 pagineNutrition and MetabolismTuTitNessuna valutazione finora
- Hipoglicemia 2020 - Ingles PDFDocumento18 pagineHipoglicemia 2020 - Ingles PDFMargaret MaggiNessuna valutazione finora
- Carbohydrate MetabolismDocumento56 pagineCarbohydrate MetabolismloijhonmuchillasNessuna valutazione finora
- TB ch24Documento11 pagineTB ch24Surajit BhattacharjeeNessuna valutazione finora
- Integration of MetabolismDocumento10 pagineIntegration of MetabolismAditya NayakNessuna valutazione finora
- Antiporda Pcoglec-Hw1midtermsDocumento5 pagineAntiporda Pcoglec-Hw1midtermsSean Antiporda100% (1)
- Nikhil BTP Mid Term ReportDocumento17 pagineNikhil BTP Mid Term ReportNikhil SaiyamNessuna valutazione finora
- программма леч. англ.Documento73 pagineпрограммма леч. англ.Rom ANessuna valutazione finora
- Importance of Carbohydrate Metabolism in Human Body: Fig.1 - Glucose StructureDocumento4 pagineImportance of Carbohydrate Metabolism in Human Body: Fig.1 - Glucose StructureRimsha EramNessuna valutazione finora
- Carbohydrate Metabolism FlashcardsDocumento84 pagineCarbohydrate Metabolism FlashcardsLejNessuna valutazione finora
- Mirjam Van Weissenbruch - Neonatal HypoglycaemiaDocumento57 pagineMirjam Van Weissenbruch - Neonatal Hypoglycaemiabenny christantoNessuna valutazione finora
- Clinical Chemistry Notes With BlanksDocumento34 pagineClinical Chemistry Notes With Blanksepson printerNessuna valutazione finora
- Biochemistry (Paper VI)Documento8 pagineBiochemistry (Paper VI)Shahidullah Kaisar ShovonNessuna valutazione finora
- GlycolysisDocumento44 pagineGlycolysisGilbert TanNessuna valutazione finora
- Mind Maps in Biochemistry - (Metabolism of Carbohydrates)Documento23 pagineMind Maps in Biochemistry - (Metabolism of Carbohydrates)Gus LionsNessuna valutazione finora
- Unit I I Carbohydrates MetabolismDocumento33 pagineUnit I I Carbohydrates Metabolismseno adi100% (2)
- Testbank Final-284-322Documento39 pagineTestbank Final-284-322khulood almerriNessuna valutazione finora
- Biochemistry Part 1Documento299 pagineBiochemistry Part 1Thelma kemiNessuna valutazione finora
- MedEntry UMAT Practice Exam Questions With Worked SolutionsDocumento88 pagineMedEntry UMAT Practice Exam Questions With Worked SolutionsMahbub AlamNessuna valutazione finora
- Nutrition and MetabolismDocumento179 pagineNutrition and Metabolismnursereview100% (9)
- Plant Biochemistry 2 RevDocumento59 paginePlant Biochemistry 2 Revenrico andrionNessuna valutazione finora
- Hormone: by Piyush Ingle Shankar BhandalkarDocumento63 pagineHormone: by Piyush Ingle Shankar BhandalkarBharatShethNessuna valutazione finora
- Biochemistry PDFDocumento114 pagineBiochemistry PDFShanmuga Moorthy100% (2)