Potrebbero piacerti anche
- Management of HypertensionDocumento64 pagineManagement of HypertensionAnonymous h0DxuJTNessuna valutazione finora
- PR MRDocumento6 paginePR MRAnonymous h0DxuJTNessuna valutazione finora
- Hemoptysis: Contribution of The Computed Tomography (CT) : CC CBGDocumento23 pagineHemoptysis: Contribution of The Computed Tomography (CT) : CC CBGAnonymous h0DxuJTNessuna valutazione finora
- Pemeriksaan Refleks BulbocavernosusDocumento2 paginePemeriksaan Refleks BulbocavernosusAnonymous h0DxuJTNessuna valutazione finora
- 712 PDFDocumento74 pagine712 PDFAnonymous h0DxuJTNessuna valutazione finora
- M 371Documento14 pagineM 371Anonymous h0DxuJTNessuna valutazione finora
- Casa Er 2015Documento12 pagineCasa Er 2015Anonymous h0DxuJTNessuna valutazione finora
- HHS Public AccessDocumento21 pagineHHS Public AccessAnonymous h0DxuJTNessuna valutazione finora
- Feeding of The Critically Ill Child-Dr. Waceke KombeDocumento22 pagineFeeding of The Critically Ill Child-Dr. Waceke KombeAnonymous h0DxuJTNessuna valutazione finora
- Nutritional Status of Children in Critical Condition at Admission To Pediatric Intensive Care UnitsDocumento6 pagineNutritional Status of Children in Critical Condition at Admission To Pediatric Intensive Care UnitsAnonymous h0DxuJTNessuna valutazione finora
- Airway Management in TraumaDocumento9 pagineAirway Management in TraumaAnonymous h0DxuJTNessuna valutazione finora
- Influence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenDocumento5 pagineInfluence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenAnonymous h0DxuJTNessuna valutazione finora
- Hard Ell 2017Documento4 pagineHard Ell 2017Anonymous h0DxuJTNessuna valutazione finora
- PXX 123Documento8 paginePXX 123Anonymous h0DxuJTNessuna valutazione finora
- Impact of Mobile Use Amongst Children in Rural Area of Marathwada Region of Maharashtra, IndiaDocumento5 pagineImpact of Mobile Use Amongst Children in Rural Area of Marathwada Region of Maharashtra, IndiaAnonymous h0DxuJTNessuna valutazione finora
- Upper Airway ManeuversDocumento9 pagineUpper Airway ManeuversAnonymous h0DxuJTNessuna valutazione finora
- Internet Scientific PublicationsDocumento12 pagineInternet Scientific PublicationsAnonymous h0DxuJTNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- AAO Reading VitrectomyDocumento65 pagineAAO Reading VitrectomydestiNessuna valutazione finora
- CGHS Rates - TrivandrumDocumento79 pagineCGHS Rates - Trivandrumimran kureshiNessuna valutazione finora
- Brochure Iolmaster 700 ModfDocumento11 pagineBrochure Iolmaster 700 ModfTT XNessuna valutazione finora
- CGHS Rates 2020 - Delhi & NCR1Documento45 pagineCGHS Rates 2020 - Delhi & NCR1ADDECC INFO INDIANessuna valutazione finora
- Devgan. Phaco Fundamentals. BookDocumento29 pagineDevgan. Phaco Fundamentals. Bookjuanjorlopez100% (3)
- Scleral-Fixated Intraocular Lens Implants-Evolution of Surgical Techniques and Future DevelopmentsDocumento32 pagineScleral-Fixated Intraocular Lens Implants-Evolution of Surgical Techniques and Future DevelopmentsHariom ShuklaNessuna valutazione finora
- Ospe Ophthalmology CorrectedDocumento55 pagineOspe Ophthalmology CorrectedGgah Vgggagagsg100% (1)
- CGHS Rates 2014 ChandigarhDocumento45 pagineCGHS Rates 2014 Chandigarhsanjeeta.chauhan22Nessuna valutazione finora
- Phacoemulsification v1Documento606 paginePhacoemulsification v1Dulnerio Sengo100% (1)
- Akash Eye Hospital - Best Eye Care Hospital in Ahmedabad, Visnagar, BharuchDocumento24 pagineAkash Eye Hospital - Best Eye Care Hospital in Ahmedabad, Visnagar, BharuchAakash Eye HospitalNessuna valutazione finora
- Biomechanical and Optical Properties of 2 New Hydrophobic Platforms For Intraocular LensesDocumento11 pagineBiomechanical and Optical Properties of 2 New Hydrophobic Platforms For Intraocular LensesJebakumarNessuna valutazione finora
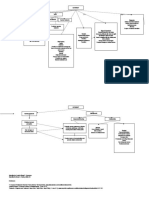
- Concept Map CATARACTDocumento2 pagineConcept Map CATARACTJrBong Semanero100% (1)
- Jogi. Mcqs-1Documento47 pagineJogi. Mcqs-1Fazan Gem100% (3)
- WEEK 17 NCS POST TEST Group 2Documento3 pagineWEEK 17 NCS POST TEST Group 2Karenkaren BescaserNessuna valutazione finora
- Approach To A Case of CataractDocumento18 pagineApproach To A Case of CataractVineet GuptaNessuna valutazione finora
- CGHS RATE List PDFDocumento42 pagineCGHS RATE List PDFNarain Kumar LangehNessuna valutazione finora
- Cmeseries 28Documento88 pagineCmeseries 28ashishNessuna valutazione finora
- Update On Optical Biometry and Intraocular Lens Power CalculationDocumento15 pagineUpdate On Optical Biometry and Intraocular Lens Power CalculationArdyNessuna valutazione finora
- Common Eye DiseasesDocumento54 pagineCommon Eye Diseaseskyro draxNessuna valutazione finora
- Alcon 2020 Corporate Responsibility ReportDocumento69 pagineAlcon 2020 Corporate Responsibility ReportRogérioNessuna valutazione finora
- IOL Power Calculation, Correction of Defocus - CH 4Documento18 pagineIOL Power Calculation, Correction of Defocus - CH 4riveliNessuna valutazione finora
- Lenstar IOLmasterDocumento6 pagineLenstar IOLmasterWillRoseroNessuna valutazione finora
- Iolmaster 4 PDFDocumento108 pagineIolmaster 4 PDFEryca TatyaneNessuna valutazione finora
- Aravind Eye Care-ShubhDocumento7 pagineAravind Eye Care-ShubhShubha Brota RahaNessuna valutazione finora
- ICL Torica ProspectoDocumento23 pagineICL Torica Prospectoajcs22Nessuna valutazione finora
- Astigmatism 2Documento35 pagineAstigmatism 2Thanujaa Uvaraj0% (1)
- Correcting Presbyopia First Phakic Diffractive IOLDocumento9 pagineCorrecting Presbyopia First Phakic Diffractive IOLFrancescFranquesaNessuna valutazione finora
- Obp PDFDocumento39 pagineObp PDFBalhansNessuna valutazione finora
- CGHS Approved Hospitals in HYDERABAD 2014Documento50 pagineCGHS Approved Hospitals in HYDERABAD 2014Priyadarshini PearlNessuna valutazione finora
- A Case Presentation of CataractDocumento16 pagineA Case Presentation of CataractDoneva Lyn Medina100% (1)