Potrebbero piacerti anche
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- For PrintingDocumento1 paginaFor PrintingHowell YapNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Compiled Case Study-LenovoDocumento24 pagineCompiled Case Study-LenovoHowell Yap100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Opd Meds Jgej PDFDocumento4 pagineOpd Meds Jgej PDFKaty SanchezNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
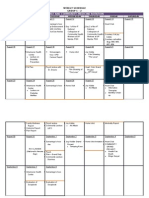
- FM Rotation Weekly Schedule Group C-2Documento2 pagineFM Rotation Weekly Schedule Group C-2Howell YapNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- W10 Water, Vitamins & MineralsDocumento37 pagineW10 Water, Vitamins & MineralsHowell YapNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- CCMH NCPDocumento7 pagineCCMH NCPajheihNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Psychiatric Nursing ReviewDocumento16 paginePsychiatric Nursing Reviewɹǝʍdןnos97% (63)
- Awakenings Video QuestionsDocumento2 pagineAwakenings Video Questionswatevermoron0% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Aging Brain, Aging MindDocumento10 pagineAging Brain, Aging MindAca AvNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Care For Clients With Physiological and Psycho Social AlterationsDocumento20 pagineCare For Clients With Physiological and Psycho Social AlterationsЯalph Basilio0% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- DementiaDocumento39 pagineDementiaAudria Graciela100% (2)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- PPD PICO Venezia Az'ZahraDocumento2 paginePPD PICO Venezia Az'ZahraMusiani Andi SudiNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Brain Bee Questions CH 1 - 11Documento13 pagineBrain Bee Questions CH 1 - 11Martyna Petrulytė88% (8)
- Abnormal Psychology Summary Matrix OF Mental Disorders: Submitted By: Fatima Anne G. DomingoDocumento45 pagineAbnormal Psychology Summary Matrix OF Mental Disorders: Submitted By: Fatima Anne G. DomingoFatima Anne G. DomingoNessuna valutazione finora
- Anti Parkinsonism DrugsDocumento8 pagineAnti Parkinsonism DrugsFaria Islam Juhi100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Chapter-2: 2.1. Process of Development of Handwriting and Its IndividualityDocumento20 pagineChapter-2: 2.1. Process of Development of Handwriting and Its IndividualityShashwat SrivastavaNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- LSVT Loud Patient Lecture Handout 2014Documento12 pagineLSVT Loud Patient Lecture Handout 2014pancho_enNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Neurologic DisordersDocumento3 pagineNeurologic Disordersjojimar08Nessuna valutazione finora
- Disautonomias Mas ComunesDocumento4 pagineDisautonomias Mas ComunesMartha DelgadoNessuna valutazione finora
- (Jeffrey L CummingsDocumento317 pagine(Jeffrey L CummingsOtilia EmaNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Resume Leaky BrainDocumento21 pagineResume Leaky Brainfelix1perez-5Nessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Med Surg A Neuro PPT 120515134413541 5Documento93 pagineMed Surg A Neuro PPT 120515134413541 5Sapiah RamanNessuna valutazione finora
- Chapter 1. History and Physical Examination - Art and ScienceDocumento3 pagineChapter 1. History and Physical Examination - Art and SciencecarolineNessuna valutazione finora
- PDDocumento29 paginePDincredible PragesNessuna valutazione finora
- Parkinson DiseaseDocumento3 pagineParkinson DiseaseBen Asiel PadangNessuna valutazione finora
- Genetice Disorders: Genetic Disorder Is A Disease or Disorder Caused by Damage or Change and Mutation On Individual's DNADocumento46 pagineGenetice Disorders: Genetic Disorder Is A Disease or Disorder Caused by Damage or Change and Mutation On Individual's DNAAna Subol AñonuevoNessuna valutazione finora
- Parkinson S DiseaseDocumento6 pagineParkinson S DiseasePratamasari InsaniNessuna valutazione finora
- Pathology MnemonicsDocumento18 paginePathology MnemonicsMamoorLatef100% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Detecting Parkinson'S Disease Using Machine LearningDocumento3 pagineDetecting Parkinson'S Disease Using Machine LearningBillo FrancisNessuna valutazione finora
- Drugs Affecting The Central Nervous SystemDocumento16 pagineDrugs Affecting The Central Nervous SystemShafaqNessuna valutazione finora
- Parkinson's UK Lincoln Branch News July 2017Documento6 pagineParkinson's UK Lincoln Branch News July 2017daniel2bratleyNessuna valutazione finora
- Quiz 12 Medical Surgical NursingDocumento14 pagineQuiz 12 Medical Surgical NursingHannahleth GorzonNessuna valutazione finora
- Royal Dutch Society For PT 2006 Guidelines For PT - Pakinson Disease PDDocumento92 pagineRoyal Dutch Society For PT 2006 Guidelines For PT - Pakinson Disease PDSiew YeeNessuna valutazione finora
- Parkinson Disease Epidemiology, Pathology, Genetics, and PathophysiologyDocumento12 pagineParkinson Disease Epidemiology, Pathology, Genetics, and PathophysiologyAna María Arenas DávilaNessuna valutazione finora
- Acn3 7 449Documento13 pagineAcn3 7 449Elisa FioraNessuna valutazione finora
- Nihms 210575Documento14 pagineNihms 210575Anakin SkywalkerNessuna valutazione finora
- NeuroSensory ExamsDocumento26 pagineNeuroSensory Examsquidditch07100% (1)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)