Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Paroles by PrevertDocumento29 pagineParoles by PrevertCity Lights90% (10)
- Trollope Mining ServicesDocumento6 pagineTrollope Mining ServicessizwehNessuna valutazione finora
- GER3620L Nov 3 09b RevDocumento60 pagineGER3620L Nov 3 09b RevGTENG CPINessuna valutazione finora
- Niche Market Tourism (Autosaved) PowerPointDocumento83 pagineNiche Market Tourism (Autosaved) PowerPointkamilahNessuna valutazione finora
- Wispeco Aluminium ProfilesDocumento22 pagineWispeco Aluminium ProfilesPatrick153Nessuna valutazione finora
- Vidagas LPGDocumento29 pagineVidagas LPGsizwehNessuna valutazione finora
- Rubis Terminal GBDocumento21 pagineRubis Terminal GBsizwehNessuna valutazione finora
- Roll Up SerrandaDocumento9 pagineRoll Up SerrandasizwehNessuna valutazione finora
- Supporting Supply Chain Planning & SchedulingDocumento8 pagineSupporting Supply Chain Planning & SchedulingsizwehNessuna valutazione finora
- Corken LPG Pumps and CompressorsDocumento24 pagineCorken LPG Pumps and Compressorssizweh100% (2)
- Mvelaphanda CircularDocumento134 pagineMvelaphanda CircularsizwehNessuna valutazione finora
- Mvela GroupDocumento97 pagineMvela GroupsizwehNessuna valutazione finora
- Mvelaserve Prelisting StatementDocumento154 pagineMvelaserve Prelisting StatementsizwehNessuna valutazione finora
- LPG AccesoriesDocumento24 pagineLPG Accesoriessizweh100% (1)
- Mocambique EIA RequirementsDocumento23 pagineMocambique EIA Requirementssizweh100% (1)
- LPG Blackmer PumpsDocumento16 pagineLPG Blackmer Pumpssizweh100% (1)
- LPG CompressorDocumento38 pagineLPG Compressorsizweh100% (1)
- LPG Vaporizer Air Mixing SystemsDocumento8 pagineLPG Vaporizer Air Mixing SystemssizwehNessuna valutazione finora
- LPG VaporizersDocumento8 pagineLPG Vaporizerssizweh100% (1)
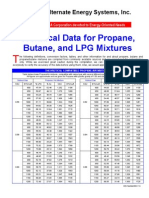
- Technical Data For LPGDocumento4 pagineTechnical Data For LPGsizwehNessuna valutazione finora
- Course CatalogueDocumento122 pagineCourse Cataloguesizweh0% (1)
- Methodology To Approve Maximum Prices For Piped GasDocumento42 pagineMethodology To Approve Maximum Prices For Piped GassizwehNessuna valutazione finora
- Sweetening LPG With AminesDocumento8 pagineSweetening LPG With AminessizwehNessuna valutazione finora
- LCMA3Documento32 pagineLCMA3sizwehNessuna valutazione finora
- Achieving Excellence Guide 2 Project OrgDocumento24 pagineAchieving Excellence Guide 2 Project OrgsizwehNessuna valutazione finora
- Appendix 1 References: LegislationDocumento12 pagineAppendix 1 References: LegislationsizwehNessuna valutazione finora
- Achieving Excellence Design QualityDocumento28 pagineAchieving Excellence Design QualitysizwehNessuna valutazione finora
- Achieving Excellence Guide 1Documento20 pagineAchieving Excellence Guide 1Leontin LeonNessuna valutazione finora
- Achievement of Market Friendly InitiativesDocumento40 pagineAchievement of Market Friendly InitiativessizwehNessuna valutazione finora
- Export Costing Sheet For Breakbulk ShipmentsDocumento15 pagineExport Costing Sheet For Breakbulk ShipmentssizwehNessuna valutazione finora
- Achieving Excellence in Construction Whole-Life Costing and Cost ManagementDocumento24 pagineAchieving Excellence in Construction Whole-Life Costing and Cost ManagementMark StankoNessuna valutazione finora
- Achieving Excellence Construction & Procurement StrategiesDocumento24 pagineAchieving Excellence Construction & Procurement Strategiessizweh100% (2)
- Stellar Nations ResumeDocumento7 pagineStellar Nations ResumeAndré Luiz CarneiroNessuna valutazione finora
- Elasticity of Demand: Managerial EconomicsDocumento41 pagineElasticity of Demand: Managerial EconomicsSomasundaram LakshminarasimhanNessuna valutazione finora
- Camisole No.8 Pattern by MyFavoriteThingsKnitwearDocumento7 pagineCamisole No.8 Pattern by MyFavoriteThingsKnitwearGarlicNessuna valutazione finora
- Marcato Capital - Letter To Lifetime Fitness BoardDocumento13 pagineMarcato Capital - Letter To Lifetime Fitness BoardCanadianValueNessuna valutazione finora
- Read Our Free Whitepaper: Philippine Supreme Court JurisprudenceDocumento32 pagineRead Our Free Whitepaper: Philippine Supreme Court JurisprudenceJoses Nino AguilarNessuna valutazione finora
- Notes Ilw1501 Introduction To LawDocumento11 pagineNotes Ilw1501 Introduction To Lawunderstand ingNessuna valutazione finora
- A Case of Uterine Fibroid Managed by Homoeopathy.20210808065707Documento5 pagineA Case of Uterine Fibroid Managed by Homoeopathy.20210808065707200408203002Nessuna valutazione finora
- Section 22 Knapsack CipherDocumento9 pagineSection 22 Knapsack CipherchitrgNessuna valutazione finora
- Coronel Vs CA, GR No 103577Documento10 pagineCoronel Vs CA, GR No 103577AddAllNessuna valutazione finora
- History of English Culture and Literature MidDocumento4 pagineHistory of English Culture and Literature Midfirdasalsa59Nessuna valutazione finora
- Agostinis Et Al-2011-CA - A Cancer Journal For CliniciansDocumento32 pagineAgostinis Et Al-2011-CA - A Cancer Journal For CliniciansKauniIsaacNessuna valutazione finora
- DerbyDB and EclipseDocumento15 pagineDerbyDB and EclipseHessa Al-AwwadNessuna valutazione finora
- Process Audit Manual 030404Documento48 pagineProcess Audit Manual 030404azadsingh1Nessuna valutazione finora
- Test 04 AnswerDocumento16 pagineTest 04 AnswerCửu KhoaNessuna valutazione finora
- Chap 005Documento13 pagineChap 005Mohammad ElabedNessuna valutazione finora
- Attitude On The Job PerformanceDocumento11 pagineAttitude On The Job PerformanceMarry Belle VidalNessuna valutazione finora
- J. C. Penney and Ron JohnsonDocumento8 pagineJ. C. Penney and Ron JohnsonadamNessuna valutazione finora
- Opening Evolution by Bill WallDocumento11 pagineOpening Evolution by Bill WallKartik ShroffNessuna valutazione finora
- Convekta Training MethodsDocumento9 pagineConvekta Training MethodsTech PadawanNessuna valutazione finora
- Dacera Vs Dela SernaDocumento2 pagineDacera Vs Dela SernaDarlo HernandezNessuna valutazione finora
- May 29Documento2 pagineMay 29gerrymattinglyNessuna valutazione finora
- Sampling TechDocumento5 pagineSampling TechJAMZ VIBESNessuna valutazione finora
- Predictor Corrector MethodsDocumento5 paginePredictor Corrector MethodsM2C7r6Nessuna valutazione finora
- ST Learning Task 10Documento6 pagineST Learning Task 10Jermaine DoloritoNessuna valutazione finora
- Grade 5 DLL Science 5 q1 Week 2aDocumento4 pagineGrade 5 DLL Science 5 q1 Week 2aTrese OliveNessuna valutazione finora
- Applied LingDocumento11 pagineApplied Lingحسام جدوNessuna valutazione finora
- Performance AnalyticsDocumento193 paginePerformance AnalyticsGNessuna valutazione finora
- Sonnet 39 ArticleDocumento2 pagineSonnet 39 ArticlelalyitaNessuna valutazione finora