Potrebbero piacerti anche
- Potato and French Fry Consumption and Risk of Type 2 Diabetes in WomenDocumento7 paginePotato and French Fry Consumption and Risk of Type 2 Diabetes in WomendarellejaideNessuna valutazione finora
- Dietary Protein and Risk of Ischemic Heart Disease in Middle-Aged Men1-3 Sarah Rosner PDocumento8 pagineDietary Protein and Risk of Ischemic Heart Disease in Middle-Aged Men1-3 Sarah Rosner Ppaulobrasil.ortopedistaNessuna valutazione finora
- LowcarbdietinwomanDocumento8 pagineLowcarbdietinwomanJoão DinizNessuna valutazione finora
- A CORRELATIVE STUDY OF RED MEAT CONSUMPTION AND CARDIO METABOLIC RISK FACTORS IN YOUNG AND AGED FEMALE PATIENTS OF TYPE 2 DIABETES DR - Satish Kumar NS1, MD, Mrs - Pavana K2, DR - Aswini Dutt R3, MDDocumento6 pagineA CORRELATIVE STUDY OF RED MEAT CONSUMPTION AND CARDIO METABOLIC RISK FACTORS IN YOUNG AND AGED FEMALE PATIENTS OF TYPE 2 DIABETES DR - Satish Kumar NS1, MD, Mrs - Pavana K2, DR - Aswini Dutt R3, MDiajpsNessuna valutazione finora
- J. Nutr.-2010-Hopping-68-74Documento7 pagineJ. Nutr.-2010-Hopping-68-74Rere RamadhanNessuna valutazione finora
- Glycemic index, glycemic load, and dietary fiber intakeDocumento9 pagineGlycemic index, glycemic load, and dietary fiber intakeAlter EgoNessuna valutazione finora
- Meat Consumption and : Red MortalityDocumento20 pagineMeat Consumption and : Red Mortalitydanielita1312Nessuna valutazione finora
- Diabetes Reversal by Plant Based Diet Dr. BiswaroopDocumento18 pagineDiabetes Reversal by Plant Based Diet Dr. BiswaroopvhirNessuna valutazione finora
- Low-Carbohydrate-Diet Score and The Risk of Coronary Heart Disease in WomenDocumento12 pagineLow-Carbohydrate-Diet Score and The Risk of Coronary Heart Disease in WomenAndrika IndrayogaNessuna valutazione finora
- Ea 55 Pustaka 13 Protein J. Nutr.-2005-Merchant-1196-201Documento6 pagineEa 55 Pustaka 13 Protein J. Nutr.-2005-Merchant-1196-201fathimzahroNessuna valutazione finora
- Prospective Study of Major Dietary Patterns and Risk of CoronaryDocumento10 pagineProspective Study of Major Dietary Patterns and Risk of CoronaryJohn SammutNessuna valutazione finora
- Adiposity Compared With Physical Inactivity and Risk of Type 2 Diabetes in WomenDocumento6 pagineAdiposity Compared With Physical Inactivity and Risk of Type 2 Diabetes in WomenEstiPramestiningtyasNessuna valutazione finora
- A Prospective Study of Egg Consumption and Risk of Cardiovascular Disease in Men and WomenDocumento8 pagineA Prospective Study of Egg Consumption and Risk of Cardiovascular Disease in Men and Womenkrazyj123Nessuna valutazione finora
- Review of LituratureDocumento12 pagineReview of Lituraturealive computerNessuna valutazione finora
- METAANALISISDocumento15 pagineMETAANALISISjotame87Nessuna valutazione finora
- 3.choi Et Al., 2005 (Purine Diet Uric Acid)Documento7 pagine3.choi Et Al., 2005 (Purine Diet Uric Acid)adrianadossantoscastNessuna valutazione finora
- Arisawa Et Al, 2014Documento12 pagineArisawa Et Al, 2014Jesana LopesNessuna valutazione finora
- LowcarbdietinmanDocumento7 pagineLowcarbdietinmanJoão DinizNessuna valutazione finora
- A Low-Fat Vegan Diet and A Conventional Diabetes Diet in The Treatment of Type 2 Diabetes: A Randomized, Controlled, 74-wk Clinical TrialDocumento9 pagineA Low-Fat Vegan Diet and A Conventional Diabetes Diet in The Treatment of Type 2 Diabetes: A Randomized, Controlled, 74-wk Clinical TrialSheldon SilvaNessuna valutazione finora
- Breakfast Cereals and Risk of Hypertension in The PhysiciansDocumento11 pagineBreakfast Cereals and Risk of Hypertension in The Physiciansclaudia ferreiraNessuna valutazione finora
- Type of Vegetarian Diet, Body Weight, and Prevalence of Type 2 DiabetesDocumento6 pagineType of Vegetarian Diet, Body Weight, and Prevalence of Type 2 DiabetesLoredana Veronica ZalischiNessuna valutazione finora
- Barnard, Et Al.,2009Documento9 pagineBarnard, Et Al.,2009Kiaraliz Rivera RosaNessuna valutazione finora
- Red meat and whole grains linked to biomarkers of diseaseDocumento9 pagineRed meat and whole grains linked to biomarkers of diseaseThalia KarampasiNessuna valutazione finora
- CHAPTER 2 by Grade 12Documento9 pagineCHAPTER 2 by Grade 12Kurt Marvin4Nessuna valutazione finora
- Paper TemplateDocumento21 paginePaper Templateapi-703153445Nessuna valutazione finora
- Peanut Consumption and Cardiovascular RiskDocumento6 paginePeanut Consumption and Cardiovascular RiskWahyuningsih HamidNessuna valutazione finora
- Patrón de Dieta Pro-Vegetariana y Mortalidad General Pro-Vegetarian Dietary Pattern and All-Cause MortalityDocumento5 paginePatrón de Dieta Pro-Vegetariana y Mortalidad General Pro-Vegetarian Dietary Pattern and All-Cause MortalityJuan Luis OlveraNessuna valutazione finora
- Dietary Saturated Fats and Their Food Sources in Relation To The RiskDocumento8 pagineDietary Saturated Fats and Their Food Sources in Relation To The RiskJohn SammutNessuna valutazione finora
- Chapter 1Documento8 pagineChapter 1Mirabete Kurt marvin - FHC1Nessuna valutazione finora
- Shahad 7Documento10 pagineShahad 7Mohammed OmarNessuna valutazione finora
- Homa B Homa IrDocumento12 pagineHoma B Homa IrMaria Marcella RusliNessuna valutazione finora
- Lectura Complementaria Carnes Rojas y Procesadas y Riesgos para La SaludDocumento7 pagineLectura Complementaria Carnes Rojas y Procesadas y Riesgos para La SaludShayAlarcónNessuna valutazione finora
- Kes Glop Aksu DiDocumento8 pagineKes Glop Aksu DiNur AnniesaNessuna valutazione finora
- Ultraprocessed Foods and Excess Heart Age Among Us AdultsDocumento10 pagineUltraprocessed Foods and Excess Heart Age Among Us AdultsSaionara FranciscoNessuna valutazione finora
- Carne en La Cena Dieta Mediterranea Tto CardiovascularDocumento1 paginaCarne en La Cena Dieta Mediterranea Tto CardiovascularDORIS JANETHNessuna valutazione finora
- NIH Public Access: Author ManuscriptDocumento22 pagineNIH Public Access: Author ManuscriptWidya PuspitaNessuna valutazione finora
- Diet Quality, Obesity and Breast Cancer Risk: An Epidemiologic Study in Córdoba, ArgentinaDocumento11 pagineDiet Quality, Obesity and Breast Cancer Risk: An Epidemiologic Study in Córdoba, ArgentinaAngelica Scherlowski FassulaNessuna valutazione finora
- Antocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Documento9 pagineAntocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Elenice Peltz NutricionistaNessuna valutazione finora
- Dietary Fiber Intake and Glycemic Control: Coronary Artery Calcification in Type 1 Diabetes (CACTI) StudyDocumento8 pagineDietary Fiber Intake and Glycemic Control: Coronary Artery Calcification in Type 1 Diabetes (CACTI) StudyLeonardo AzevedoNessuna valutazione finora
- Chapter 2 - Grade 12 He3 (Setb Backsub)Documento6 pagineChapter 2 - Grade 12 He3 (Setb Backsub)Mirabete Kurt marvin - FHC1Nessuna valutazione finora
- Meal Frequency and Timing Are Associated With Changes in Body Mass Index in Adventist Health Study 2Documento7 pagineMeal Frequency and Timing Are Associated With Changes in Body Mass Index in Adventist Health Study 2Cristi CapetisNessuna valutazione finora
- Mattei-2011-A Meat Processed Meat and French Fries Dietary Pattern Is Associated With High Allostatic Load in Puerto Rican Older AdultsDocumento9 pagineMattei-2011-A Meat Processed Meat and French Fries Dietary Pattern Is Associated With High Allostatic Load in Puerto Rican Older AdultsluizfernandosellaNessuna valutazione finora
- Purine-Rich Foods, Dairy and Protein Intake, and The Risk of Gout in MenDocumento11 paginePurine-Rich Foods, Dairy and Protein Intake, and The Risk of Gout in MenAttila TamasNessuna valutazione finora
- Important Factors in Managing Diabetes and Preventing Its Long-Term ComplicationsresearchDocumento2 pagineImportant Factors in Managing Diabetes and Preventing Its Long-Term Complicationsresearchstanleec34Nessuna valutazione finora
- Nutritional Status Among Women With Pre-Eclampsia and Healthy Pregnant and Non-Pregnant Women in A Latin American CountryDocumento7 pagineNutritional Status Among Women With Pre-Eclampsia and Healthy Pregnant and Non-Pregnant Women in A Latin American CountryAchmad Deza FaristaNessuna valutazione finora
- Dietary Fat Modifies The Effects of FTO Genotype On Changes in Insulin Sensitivity.Documento6 pagineDietary Fat Modifies The Effects of FTO Genotype On Changes in Insulin Sensitivity.Christian Jovanni Flores SolisNessuna valutazione finora
- Sự Gia Tăng Protein Trong Chế Độ Ăn Uống Giúp Cải Thiện Phản Ứng Đường Huyết ở Những Người Mắc Bệnh Tiểu Đường Loại 2Documento8 pagineSự Gia Tăng Protein Trong Chế Độ Ăn Uống Giúp Cải Thiện Phản Ứng Đường Huyết ở Những Người Mắc Bệnh Tiểu Đường Loại 2Cao Phát ĐạtNessuna valutazione finora
- Glycemic ControlDocumento5 pagineGlycemic ControlFxStuntDriverNessuna valutazione finora
- Dietary Flavonoid Intake and Weight Maintenance: Three Prospective Cohorts of 124 086 US Men and Women Followed For Up To 24 YearsDocumento7 pagineDietary Flavonoid Intake and Weight Maintenance: Three Prospective Cohorts of 124 086 US Men and Women Followed For Up To 24 YearsRasha Samir SryoNessuna valutazione finora
- Mortality in British Vegetarians: Paul N Appleby, Timothy J Key, Margaret Thorogood, Michael L Burr and Jim MannDocumento8 pagineMortality in British Vegetarians: Paul N Appleby, Timothy J Key, Margaret Thorogood, Michael L Burr and Jim Mannluis11256Nessuna valutazione finora
- Nej Mo A 1304501aasDocumento12 pagineNej Mo A 1304501aasHadiyana Arief HafizNessuna valutazione finora
- Ultra Processed Foods and Cardiovascular Diseases Poten - 2021 - Advances in NuDocumento8 pagineUltra Processed Foods and Cardiovascular Diseases Poten - 2021 - Advances in NuMauricio RebolloNessuna valutazione finora
- Vegetarian, Vegan Diets Linked to Lower Heart Disease, Cancer RiskDocumento50 pagineVegetarian, Vegan Diets Linked to Lower Heart Disease, Cancer RiskFilipa FerreiraNessuna valutazione finora
- REDALYGDocumento8 pagineREDALYGjoel cedeño SánchezNessuna valutazione finora
- 2 Year Paleo TrialDocumento8 pagine2 Year Paleo TrialOfer KulkaNessuna valutazione finora
- Am. J. Epidemiol.-2003-Ma-85-92Documento8 pagineAm. J. Epidemiol.-2003-Ma-85-92Eima Siti NurimahNessuna valutazione finora
- Low-Carbohydrate, High-Protein Score and Mortality in A Northern Swedish Population-Based CohortDocumento8 pagineLow-Carbohydrate, High-Protein Score and Mortality in A Northern Swedish Population-Based CohorthernaputraNessuna valutazione finora
- Dieta Vegana y DiabetesDocumento7 pagineDieta Vegana y DiabetesPAUL ANDRES CHAMBA MOLINANessuna valutazione finora
- The China Study: The Most Comprehensive Study of Nutrition Ever Conducted and the Startling Implications for Diet, Weight Loss and Long-term Health by T. Colin Campbell and Thomas M. Campbell, II | Key Takeaways, Analysis & ReviewDa EverandThe China Study: The Most Comprehensive Study of Nutrition Ever Conducted and the Startling Implications for Diet, Weight Loss and Long-term Health by T. Colin Campbell and Thomas M. Campbell, II | Key Takeaways, Analysis & ReviewValutazione: 5 su 5 stelle5/5 (1)
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsDa EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNessuna valutazione finora
- Links de Registro en ExchangesDocumento4 pagineLinks de Registro en ExchangestedescofedericoNessuna valutazione finora
- LogDocumento1 paginaLogtedescofedericoNessuna valutazione finora
- LogDocumento1 paginaLogtedescofedericoNessuna valutazione finora
- Mod4 Type 2 Diabetes Vegetarian DietDocumento7 pagineMod4 Type 2 Diabetes Vegetarian DiettedescofedericoNessuna valutazione finora
- Release NoteDocumento1 paginaRelease NotetedescofedericoNessuna valutazione finora
- Mod5 Incidence OsteoporosisDocumento4 pagineMod5 Incidence OsteoporosistedescofedericoNessuna valutazione finora
- Mod5 Dairy FoodsDocumento9 pagineMod5 Dairy FoodstedescofedericoNessuna valutazione finora
- Mod4 Associationes Diet CancerDocumento7 pagineMod4 Associationes Diet CancertedescofedericoNessuna valutazione finora
- Mod5 Health DiseaseDocumento6 pagineMod5 Health DiseasetedescofedericoNessuna valutazione finora
- Mod4 Cardiovascular Renal BenefitsDocumento11 pagineMod4 Cardiovascular Renal BenefitstedescofedericoNessuna valutazione finora
- Ebook Digital DownloadDocumento33 pagineEbook Digital DownloadtedescofedericoNessuna valutazione finora
- Mod4 Red Meat Type 2 DiabetesDocumento8 pagineMod4 Red Meat Type 2 DiabetestedescofedericoNessuna valutazione finora
- Mod3 11 Academic Medical Center Response To Childhood ObesityDocumento6 pagineMod3 11 Academic Medical Center Response To Childhood ObesitytedescofedericoNessuna valutazione finora
- Mod4 Nut Corn PopcornDocumento9 pagineMod4 Nut Corn PopcorntedescofedericoNessuna valutazione finora
- Mod4 Diet and Bone HealthDocumento31 pagineMod4 Diet and Bone HealthtedescofedericoNessuna valutazione finora
- Parcial Regimen Penal AduaneroDocumento6 pagineParcial Regimen Penal AduaneroFederico TedescoNessuna valutazione finora
- Vitamin B Status, Deficiency and Its Consequences - An OverviewDocumento18 pagineVitamin B Status, Deficiency and Its Consequences - An OverviewtedescofedericoNessuna valutazione finora
- Mod4 Type 2 Diabetes Vegetarian DietDocumento7 pagineMod4 Type 2 Diabetes Vegetarian DiettedescofedericoNessuna valutazione finora
- Vitamin B Status, Deficiency and Its Consequences - An OverviewDocumento18 pagineVitamin B Status, Deficiency and Its Consequences - An OverviewtedescofedericoNessuna valutazione finora
- Abstract and Introduction: Laurie Dunham, MS, RD, LD Linda M. Kollar, RN, MSNDocumento13 pagineAbstract and Introduction: Laurie Dunham, MS, RD, LD Linda M. Kollar, RN, MSNtedescofedericoNessuna valutazione finora
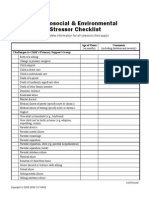
- Mod3 10 Psychosocial and Environmental Stressor ChecklistDocumento3 pagineMod3 10 Psychosocial and Environmental Stressor ChecklisttedescofedericoNessuna valutazione finora
- Vegsocorg Parentteenager Guidebook ColgarDocumento19 pagineVegsocorg Parentteenager Guidebook ColgartedescofedericoNessuna valutazione finora
- Hartman Validity StudiesDocumento28 pagineHartman Validity StudiestedescofedericoNessuna valutazione finora
- Parcial Regimen Penal AduaneroDocumento6 pagineParcial Regimen Penal AduaneroFederico TedescoNessuna valutazione finora
- TWAIN32Documento1 paginaTWAIN32tedescofedericoNessuna valutazione finora
- Do You Binge EatDocumento1 paginaDo You Binge EattedescofedericoNessuna valutazione finora
- Iron DeficiencyDocumento15 pagineIron DeficiencytedescofedericoNessuna valutazione finora
- Eat Mindfully, Live Vibrantly: Michelle May, M.DDocumento2 pagineEat Mindfully, Live Vibrantly: Michelle May, M.DtedescofedericoNessuna valutazione finora
- Am I Hungry Facilitator TrainingDocumento14 pagineAm I Hungry Facilitator TrainingtedescofedericoNessuna valutazione finora