Potrebbero piacerti anche
- Biomolecules 12 00066Documento10 pagineBiomolecules 12 00066holmessbNessuna valutazione finora
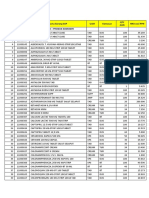
- No. Kode Sap Nama Barang Sap Uom Kemasan Qty Aun Hna Excl PPN Lini Produk: Ogb + Produk KomoditiDocumento4 pagineNo. Kode Sap Nama Barang Sap Uom Kemasan Qty Aun Hna Excl PPN Lini Produk: Ogb + Produk KomoditiholmessbNessuna valutazione finora
- 2405 4477 1 SMDocumento1 pagina2405 4477 1 SMholmessbNessuna valutazione finora
- 1991 BP Nazareth EtalDocumento6 pagine1991 BP Nazareth EtalholmessbNessuna valutazione finora
- Advances Vol3 6 Detox AntioxidantsDocumento6 pagineAdvances Vol3 6 Detox AntioxidantsholmessbNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Msds CatDocumento7 pagineMsds CatraniNessuna valutazione finora
- 478 PeriodizationDocumento13 pagine478 Periodizationomarou1867% (3)
- Steven Franklin Greer 1 PDFDocumento136 pagineSteven Franklin Greer 1 PDFWKYC.comNessuna valutazione finora
- PI - Standard - Seafood Processing - Issue 5.0 - 1-February-2019Documento65 paginePI - Standard - Seafood Processing - Issue 5.0 - 1-February-2019pebru yuwono0% (1)
- NCP Acute Pain Related To Tissue Ischemia As Manifested by Changes in Level of Consciousness PDFDocumento3 pagineNCP Acute Pain Related To Tissue Ischemia As Manifested by Changes in Level of Consciousness PDFOGNTVNessuna valutazione finora
- IntroductionDocumento9 pagineIntroductionMarc Harold FloresNessuna valutazione finora
- PayseptDocumento1 paginaPayseptJasmine SinglaNessuna valutazione finora
- Relationship Among Levels of DFDsDocumento8 pagineRelationship Among Levels of DFDssunny_242574Nessuna valutazione finora
- Republic Act No. 11210 - 105-Day Expanded Maternity Leave LawDocumento4 pagineRepublic Act No. 11210 - 105-Day Expanded Maternity Leave LawRaymond CruzinNessuna valutazione finora
- Pan India WED Report 21Documento162 paginePan India WED Report 21nioh envisNessuna valutazione finora
- Surgeons in Rangpur, Bangladesh - SOSBDocumento11 pagineSurgeons in Rangpur, Bangladesh - SOSBWadood Md ZahedNessuna valutazione finora
- FV2113 Short Note Student Copy Assignmnet 1 (1) 2000Documento9 pagineFV2113 Short Note Student Copy Assignmnet 1 (1) 2000Nadia RiazNessuna valutazione finora
- Risk Factors of Internet Addiction Among AdolescentsDocumento14 pagineRisk Factors of Internet Addiction Among AdolescentsM. F. MubinNessuna valutazione finora
- Psychological Well Being - 18 ItemsDocumento5 paginePsychological Well Being - 18 ItemsIqra LatifNessuna valutazione finora
- Cummins Prem Blue 15w40 1-18 L Sing Ssv3028m18 Asia-Pacific Purple Book (GHS) - EnglishDocumento14 pagineCummins Prem Blue 15w40 1-18 L Sing Ssv3028m18 Asia-Pacific Purple Book (GHS) - EnglishjosephvanbacNessuna valutazione finora
- Delirium Using The 4AT AssessmentDocumento10 pagineDelirium Using The 4AT AssessmentAna KmaidNessuna valutazione finora
- Caroline O'Mahony Caroline's Fit PlanDocumento30 pagineCaroline O'Mahony Caroline's Fit PlanGizem MutluNessuna valutazione finora
- Stress Management Stress Management: NptelDocumento99 pagineStress Management Stress Management: NptelDKNessuna valutazione finora
- TUM CoursesDocumento3 pagineTUM CoursesJoao N Da SilvaNessuna valutazione finora
- Draft Resolution ExampleDocumento8 pagineDraft Resolution ExampleAyutasariNessuna valutazione finora
- Magnetis Polus AmboDocumento4 pagineMagnetis Polus Amboadi.mititean1585Nessuna valutazione finora
- Lesson Plan in Phylum Protozoa G8Documento4 pagineLesson Plan in Phylum Protozoa G8Jeanacela PagaspasNessuna valutazione finora
- Antinociceptic Activity of Talisay ExtractDocumento22 pagineAntinociceptic Activity of Talisay ExtractRein Paul Pascua TomasNessuna valutazione finora
- Thesis Dental ImplantsDocumento4 pagineThesis Dental Implantstmexyhikd100% (2)
- Masha Sardari Nutrition ResumeDocumento2 pagineMasha Sardari Nutrition Resumeapi-428097674Nessuna valutazione finora
- The Tactical Combat Casualty Care Casualty Card - TCCC Guidelines - Proposed Change 1301Documento9 pagineThe Tactical Combat Casualty Care Casualty Card - TCCC Guidelines - Proposed Change 1301Paschalis DevranisNessuna valutazione finora
- New Trends in Mechanical VentilationDocumento4 pagineNew Trends in Mechanical Ventilationashley_castro_4Nessuna valutazione finora
- Mental and Emotional Health PowerpointDocumento36 pagineMental and Emotional Health PowerpointYen Aduana86% (7)
- Physical Assessment For Stroke PatientDocumento4 paginePhysical Assessment For Stroke Patientdana75% (4)
- Summary of Non Sexist CityDocumento2 pagineSummary of Non Sexist CityIMY KARDAS100% (3)