Potrebbero piacerti anche
- Pollution Control in Oil, Gas and Chemical PlantsDa EverandPollution Control in Oil, Gas and Chemical PlantsNessuna valutazione finora
- Handbook of Air Pollution Prevention and ControlDa EverandHandbook of Air Pollution Prevention and ControlValutazione: 5 su 5 stelle5/5 (2)
- Hospital HVAC Design A Challenge For IAQ, Energy Recovery and System Reliability - Issue Jul-Sep 2002Documento11 pagineHospital HVAC Design A Challenge For IAQ, Energy Recovery and System Reliability - Issue Jul-Sep 2002Go Tze FongNessuna valutazione finora
- ASHRAE Rousseau Et AlDocumento5 pagineASHRAE Rousseau Et AlSantanu DasNessuna valutazione finora
- HVAC in Hospital PDFDocumento7 pagineHVAC in Hospital PDFMohammed Toema100% (1)
- Energy Conservation: ASHRAE Standard 90.1. Each New BuildingDocumento4 pagineEnergy Conservation: ASHRAE Standard 90.1. Each New BuildingdemuthuNessuna valutazione finora
- Ventilation Calculation 1 PDFDocumento5 pagineVentilation Calculation 1 PDFGior GioNessuna valutazione finora
- Ides-Edu: Lecture 7: Sizing Natural Ventilation SystemsDocumento17 pagineIdes-Edu: Lecture 7: Sizing Natural Ventilation Systemsabhijeet7362Nessuna valutazione finora
- OR Ventilation Systems GuideDocumento6 pagineOR Ventilation Systems GuideJuan IntriagoNessuna valutazione finora
- New Method for Calculating Evaporation from Occupied PoolsDocumento4 pagineNew Method for Calculating Evaporation from Occupied PoolsSarosh MohiyuddinNessuna valutazione finora
- Ventilation RatesDocumento4 pagineVentilation RatesReza KhajeNessuna valutazione finora
- Vertical Plumbing Overcomes Space LimitationsDocumento4 pagineVertical Plumbing Overcomes Space Limitationsexfireex2Nessuna valutazione finora
- Air Diffusion Performance Index (ADPI) of Diffusers For Heating ModeDocumento21 pagineAir Diffusion Performance Index (ADPI) of Diffusers For Heating ModeAlbert Aromin EngrNessuna valutazione finora
- 200911ceu 162Documento7 pagine200911ceu 162Mohamed Mostafa AamerNessuna valutazione finora
- Acoustic Ventilation BrochureDocumento10 pagineAcoustic Ventilation BrochureraghuragooNessuna valutazione finora
- NEW FGI Residential Guidelines PDFDocumento327 pagineNEW FGI Residential Guidelines PDFzahidNessuna valutazione finora
- Ducts DetailsDocumento8 pagineDucts DetailsfayasNessuna valutazione finora
- Hvac System Control & OptimizationDocumento27 pagineHvac System Control & OptimizationSHAHAB SAQUIBNessuna valutazione finora
- TD 6 - Design CalculationsDocumento25 pagineTD 6 - Design CalculationsKim Angelique PerialdeNessuna valutazione finora
- Domestic Ventilation SolutionsDocumento20 pagineDomestic Ventilation SolutionsDraganNessuna valutazione finora
- Principles and Concepts of Laboratory DesignDocumento6 paginePrinciples and Concepts of Laboratory DesignVu ToanNessuna valutazione finora
- Smoke MovementDocumento13 pagineSmoke Movementzshehadeh100% (2)
- Continuing Education From Plumbing Systems & DesignDocumento362 pagineContinuing Education From Plumbing Systems & DesignSchreiber_DiesesNessuna valutazione finora
- Hospital Designs in Tropical Malaysia Towards a Greener AgendaDocumento47 pagineHospital Designs in Tropical Malaysia Towards a Greener AgendaAlex ChinNessuna valutazione finora
- HMDA Mechanical Services Data Book Medical Gas Systems 2021 Edition 1 Sources of SupplyDocumento10 pagineHMDA Mechanical Services Data Book Medical Gas Systems 2021 Edition 1 Sources of SupplyeimrehNessuna valutazione finora
- Calculating Evaporation Swimming PoolsDocumento3 pagineCalculating Evaporation Swimming PoolsSyed Munawar AliNessuna valutazione finora
- ASHRAE 62.1 and LEED Ventilation RequirementsDocumento41 pagineASHRAE 62.1 and LEED Ventilation RequirementsAndreAPLNessuna valutazione finora
- A Designer's Guide To The Options For Ventilation and CoolingDocumento40 pagineA Designer's Guide To The Options For Ventilation and CoolingSonny RamosNessuna valutazione finora
- 12international Healthcare Building Standards Codes - Henning LenschDocumento69 pagine12international Healthcare Building Standards Codes - Henning LenschAl Dizdar NazarNessuna valutazione finora
- Advantage Disadvangtage of Suspended Vs Open CeilingDocumento5 pagineAdvantage Disadvangtage of Suspended Vs Open CeilingAre OnezNessuna valutazione finora
- Handbook of Smoke Control EngineeringDocumento1 paginaHandbook of Smoke Control Engineeringskywalker_handsome50% (2)
- Humidity Control - Hospital Operating Room DehumidificationDocumento6 pagineHumidity Control - Hospital Operating Room Dehumidificationengamer80100% (1)
- Heat Ventilation and Air Conditioning (HVAC)Documento46 pagineHeat Ventilation and Air Conditioning (HVAC)Sagar GoyalNessuna valutazione finora
- Medical Gas Pipeline SizingDocumento6 pagineMedical Gas Pipeline Sizingnini26100% (3)
- Ashrae D62Documento27 pagineAshrae D62Amro Metwally El HendawyNessuna valutazione finora
- Save up to 80% on HVAC Energy Costs with Heat Recovery UnitsDocumento35 pagineSave up to 80% on HVAC Energy Costs with Heat Recovery UnitsGabetsos KaraflidisNessuna valutazione finora
- Air Distribution Engg GuideDocumento8 pagineAir Distribution Engg GuideNiong DavidNessuna valutazione finora
- Cooling Load Calc PBL PDFDocumento14 pagineCooling Load Calc PBL PDFkunal jatharNessuna valutazione finora
- Fdocuments - in Ariston Water Heater CatalogueDocumento68 pagineFdocuments - in Ariston Water Heater CatalogueMahmoudNessuna valutazione finora
- Fan Coil Unit: Design and OperationDocumento6 pagineFan Coil Unit: Design and OperationbetteroneNessuna valutazione finora
- HPAC Article On Specifying VAV BoxesDocumento4 pagineHPAC Article On Specifying VAV Boxesjoejex123Nessuna valutazione finora
- Xpelair Ventilation Guide - EngDocumento63 pagineXpelair Ventilation Guide - EngMarc MaesNessuna valutazione finora
- Acoustic of Green BuildingsDocumento7 pagineAcoustic of Green BuildingsJuan DupezhNessuna valutazione finora
- Ashrae Standard 62-1989 DesignDocumento1 paginaAshrae Standard 62-1989 DesignDuxToyNessuna valutazione finora
- Q T - O P: Mechanical Engineering and IndustryDocumento20 pagineQ T - O P: Mechanical Engineering and IndustrysamehNessuna valutazione finora
- Health Facilities Design 2010 FGI GuidelinesDocumento79 pagineHealth Facilities Design 2010 FGI GuidelinesAbu Talha FarooqiNessuna valutazione finora
- MECH3423 - 1516 - 08-Mechanical and Natural VentilationDocumento53 pagineMECH3423 - 1516 - 08-Mechanical and Natural Ventilationahtin618Nessuna valutazione finora
- NACO Duideline For BSL2 LabDocumento27 pagineNACO Duideline For BSL2 Labdamadol100% (1)
- Air Change CFM CalculatorDocumento1 paginaAir Change CFM CalculatorAbdul Mohid SheikhNessuna valutazione finora
- Cibse Swimming PoolpdfDocumento13 pagineCibse Swimming PoolpdfBao Loc DuongNessuna valutazione finora
- HVAC - Overview of Space Heating Systems PDFDocumento68 pagineHVAC - Overview of Space Heating Systems PDFFredie UnabiaNessuna valutazione finora
- Germany Guideline SBDocumento123 pagineGermany Guideline SBlockas222Nessuna valutazione finora
- Tutorial - Underfloor Air-ConditioningDocumento8 pagineTutorial - Underfloor Air-ConditioningJasper_HVACNessuna valutazione finora
- Vacuum Aerosol 4Documento10 pagineVacuum Aerosol 4khamilatusyNessuna valutazione finora
- Journal of Dentistry: SciencedirectDocumento9 pagineJournal of Dentistry: SciencedirectkittyNessuna valutazione finora
- Perchloroethylene (PERC) in Dry Cleaning: Reducing Worker Exposure ToDocumento28 paginePerchloroethylene (PERC) in Dry Cleaning: Reducing Worker Exposure ToSenthil KumarNessuna valutazione finora
- Macam Isolasi TambahanDocumento2 pagineMacam Isolasi TambahanDella SufyNessuna valutazione finora
- Atmosphric PollutionDocumento10 pagineAtmosphric Pollutionعلي الاسديNessuna valutazione finora
- Aerosoles GlosarioDocumento2 pagineAerosoles GlosarioBJ CarminatorNessuna valutazione finora
- Uktra Clean OTsDocumento8 pagineUktra Clean OTshadianatyaNessuna valutazione finora
- p353 PDFDocumento6 paginep353 PDFShkelzen KomoniNessuna valutazione finora
- Ftesa Anglisht Per SimpoziumDocumento2 pagineFtesa Anglisht Per SimpoziumShkelzen KomoniNessuna valutazione finora
- The Antimicrobial Effect of Diode Laser With Heat Producing Toward E PDFDocumento1 paginaThe Antimicrobial Effect of Diode Laser With Heat Producing Toward E PDFShkelzen KomoniNessuna valutazione finora
- Advances in Life Science and TechnologyDocumento2 pagineAdvances in Life Science and TechnologyShkelzen KomoniNessuna valutazione finora
- Thyroglossal Duct Remnants-1 PDFDocumento6 pagineThyroglossal Duct Remnants-1 PDFShkelzen KomoniNessuna valutazione finora
- Devitec 11402Documento1 paginaDevitec 11402Shkelzen KomoniNessuna valutazione finora
- Submandibular Gland Excision PDFDocumento7 pagineSubmandibular Gland Excision PDFnandhinisankaranNessuna valutazione finora
- Maat 07 I 1 P 85Documento3 pagineMaat 07 I 1 P 85Shkelzen KomoniNessuna valutazione finora
- CondyleBookChapter3 PDFDocumento6 pagineCondyleBookChapter3 PDFShkelzen KomoniNessuna valutazione finora
- Ranula and Sublingual Salivary Gland ExcisionDocumento5 pagineRanula and Sublingual Salivary Gland Excisionasep budiyantoNessuna valutazione finora
- Joint Pain Leaflet PDFDocumento12 pagineJoint Pain Leaflet PDFSuaeni Kurnia Wirda100% (1)
- Tooth PreservationDocumento16 pagineTooth PreservationShkelzen KomoniNessuna valutazione finora
- Soft Tissue Enhancement Around Dental ImplantDocumento20 pagineSoft Tissue Enhancement Around Dental ImplantWang KaiminNessuna valutazione finora
- Posters FinalDocumento70 paginePosters FinalShkelzen KomoniNessuna valutazione finora
- Operatory Packages14 LRDocumento8 pagineOperatory Packages14 LRShkelzen KomoniNessuna valutazione finora
- Dicom Questionnaire v3.2Documento10 pagineDicom Questionnaire v3.2Shkelzen KomoniNessuna valutazione finora
- Overview of Pulpal ProtectionDocumento13 pagineOverview of Pulpal ProtectionkeralaappleNessuna valutazione finora
- Tooth PreservationDocumento16 pagineTooth PreservationShkelzen KomoniNessuna valutazione finora
- Material Safety Data Sheet: Product IdentificationDocumento2 pagineMaterial Safety Data Sheet: Product Identificationمحمد عزتNessuna valutazione finora
- Con4156 Ans Very ImportantDocumento6 pagineCon4156 Ans Very ImportantGordon0123Nessuna valutazione finora
- Case Study Residential Building PresentationDocumento26 pagineCase Study Residential Building PresentationAyushree RajbhandariNessuna valutazione finora
- The Factories Act, 1948Documento60 pagineThe Factories Act, 1948Pavan RaiNessuna valutazione finora
- Hvac Design Manual: First EditionDocumento124 pagineHvac Design Manual: First EditionNathan Tom100% (6)
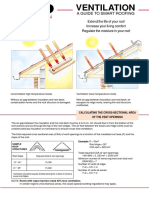
- Smart Roof Ventilation GuideDocumento1 paginaSmart Roof Ventilation GuideBogdan RuxandaNessuna valutazione finora
- Chapter 5: Preheat: 5.1. Theory and ApplicationsDocumento7 pagineChapter 5: Preheat: 5.1. Theory and Applicationslang74Nessuna valutazione finora
- Sg22e Gas Convection Oven Vhl002-2bDocumento47 pagineSg22e Gas Convection Oven Vhl002-2bGabino Ubilio MurilloNessuna valutazione finora
- Air Inlet, Exhaust, Ventilation SystemsDocumento5 pagineAir Inlet, Exhaust, Ventilation SystemsnayearNessuna valutazione finora
- CefdinirDocumento7 pagineCefdinirabanoub melekNessuna valutazione finora
- CKV Design Guide 1 031504 PDFDocumento21 pagineCKV Design Guide 1 031504 PDFThanasis TsellosNessuna valutazione finora
- Calor Equipo SDocumento604 pagineCalor Equipo SchylergNessuna valutazione finora
- HKIAQDocumento84 pagineHKIAQHei Kan ChengNessuna valutazione finora
- Is 3034 - 1993 (1998 - Fire Protection For Thermal Power Plants)Documento20 pagineIs 3034 - 1993 (1998 - Fire Protection For Thermal Power Plants)satnam1979100% (2)
- HVAC CommissioningDocumento27 pagineHVAC CommissioningSADJI RachidNessuna valutazione finora
- Intelligent InteriorsDocumento9 pagineIntelligent InteriorsMaria IqbalNessuna valutazione finora
- Pmz3 Engineering Manual 2011Documento35 paginePmz3 Engineering Manual 2011bigcountry1963Nessuna valutazione finora
- Available StandardsDocumento26 pagineAvailable StandardsZaki AnwerNessuna valutazione finora
- Checklist For Case Study - 2018 - 19 PDFDocumento3 pagineChecklist For Case Study - 2018 - 19 PDFMohamed Basil AliNessuna valutazione finora
- Passive Climate Design Heritage BuildingsDocumento20 paginePassive Climate Design Heritage Buildingsatharvasaxena93Nessuna valutazione finora
- 2002-9001-005EN0513 Barn Cleaner - Instrution ManualDocumento86 pagine2002-9001-005EN0513 Barn Cleaner - Instrution ManualGabriel RusuNessuna valutazione finora
- Cooling Load Reduction by Using Thermal Mass and Night Ventilation PDFDocumento7 pagineCooling Load Reduction by Using Thermal Mass and Night Ventilation PDFSérgio GnipperNessuna valutazione finora
- Roldan, MC (400 Questions)Documento68 pagineRoldan, MC (400 Questions)Couline Castillo Roldan - DinoyNessuna valutazione finora
- Fans.: Mechanical VentilationDocumento6 pagineFans.: Mechanical VentilationAnwesha PanigrahiNessuna valutazione finora
- Testing Staircase PressurizationDocumento5 pagineTesting Staircase Pressurizationthanhlamndl100% (1)
- Manufacturing of AcetyleneDocumento45 pagineManufacturing of Acetylenebecpavan100% (1)
- Climate-Responsive Features of Rajasthan Heritage ArchitectureDocumento8 pagineClimate-Responsive Features of Rajasthan Heritage ArchitectureMohammad AzharuddinNessuna valutazione finora
- Backdraft 04 ENGDocumento5 pagineBackdraft 04 ENGForum PompieriiNessuna valutazione finora
- ASHRAE Journal - LEED and Standard 62.1-TaylorDocumento4 pagineASHRAE Journal - LEED and Standard 62.1-TaylorNg Khanh100% (1)