Potrebbero piacerti anche
- TransportationDocumento1 paginaTransportationAqilah MahabirNessuna valutazione finora
- ErgonomicsDocumento4 pagineErgonomicsSubhashini RajshekarNessuna valutazione finora
- Redox 2Documento8 pagineRedox 2Aqilah MahabirNessuna valutazione finora
- Cxcpastpaper 1 June 2010Documento11 pagineCxcpastpaper 1 June 2010Aqilah MahabirNessuna valutazione finora
- Dental Ergonomics To Combat MSDSDocumento11 pagineDental Ergonomics To Combat MSDSAqilah MahabirNessuna valutazione finora
- Erg in DentDocumento5 pagineErg in DentAqilah MahabirNessuna valutazione finora
- Dentistry 2 1032Documento4 pagineDentistry 2 1032Aqilah MahabirNessuna valutazione finora
- Ergonomics and Dental WorkDocumento29 pagineErgonomics and Dental WorkNicu Ciobanu100% (5)
- Work-Related Musculoskeletal Disorders Among Health Care Professionals - A Cross-Sectional Assessment of Risk Factors in A Tertiary Hospital, IndiaDocumento14 pagineWork-Related Musculoskeletal Disorders Among Health Care Professionals - A Cross-Sectional Assessment of Risk Factors in A Tertiary Hospital, IndiaAqilah MahabirNessuna valutazione finora
- English For Csec PAPER 1 (1 Hour 30 Minutes) - 60 Multiple Choice ItemsDocumento2 pagineEnglish For Csec PAPER 1 (1 Hour 30 Minutes) - 60 Multiple Choice ItemsAqilah MahabirNessuna valutazione finora
- Prevalence of Musculoskeletal Disorders in Dentists) PDFDocumento8 paginePrevalence of Musculoskeletal Disorders in Dentists) PDFAqilah MahabirNessuna valutazione finora
- Ergonomic ConsiderationsDocumento17 pagineErgonomic ConsiderationsAqilah MahabirNessuna valutazione finora
- Supplementary Information: Table S1. The Basic Hygiene Information of 13 Factories Participated in This StudyDocumento5 pagineSupplementary Information: Table S1. The Basic Hygiene Information of 13 Factories Participated in This StudyAqilah MahabirNessuna valutazione finora
- A Systematic Review of MsdsDocumento7 pagineA Systematic Review of MsdsAqilah MahabirNessuna valutazione finora
- Dentistry 2 1032Documento4 pagineDentistry 2 1032Aqilah MahabirNessuna valutazione finora
- Airflow FormulasDocumento4 pagineAirflow FormulasYoesof HilabyNessuna valutazione finora
- CDA ErgonimicsDocumento49 pagineCDA ErgonimicsAqilah MahabirNessuna valutazione finora
- Ergonomics For THE 21 Century: Office of Risk Management Loss Prevention UnitDocumento90 pagineErgonomics For THE 21 Century: Office of Risk Management Loss Prevention UnitBalaji ManivelNessuna valutazione finora
- Ergonomics PaperDocumento26 pagineErgonomics Paperjaymin1Nessuna valutazione finora
- Erg in DentDocumento5 pagineErg in DentAqilah MahabirNessuna valutazione finora
- HPLC LCMS Lab ReportDocumento3 pagineHPLC LCMS Lab ReportAqilah Mahabir100% (1)
- Ozone DepletionDocumento18 pagineOzone DepletionAqilah MahabirNessuna valutazione finora
- Causes of The Global Warming Observed Since The 19th CenturyDocumento15 pagineCauses of The Global Warming Observed Since The 19th CenturyAqilah MahabirNessuna valutazione finora
- Soil Remediation - Appearances Can Be DeceivingDocumento5 pagineSoil Remediation - Appearances Can Be DeceivingAqilah MahabirNessuna valutazione finora
- ThesisDocumento169 pagineThesisAqilah MahabirNessuna valutazione finora
- Symmetry and Group TheoryDocumento129 pagineSymmetry and Group TheoryMatthew HansenNessuna valutazione finora
- Nozik 2008 Multiple Exciton Generation in Semiconductor Quantum DotsDocumento9 pagineNozik 2008 Multiple Exciton Generation in Semiconductor Quantum DotsAqilah MahabirNessuna valutazione finora
- Kang+etal SCIENCE 2011Documento4 pagineKang+etal SCIENCE 2011Aqilah MahabirNessuna valutazione finora
- 41741Documento6 pagine41741Aqilah MahabirNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Prices & Services Updates: DashboardDocumento1 paginaPrices & Services Updates: Dashboardzafira fatimaNessuna valutazione finora
- Interference Fit Calculation GuideDocumento23 pagineInterference Fit Calculation GuideEMRENessuna valutazione finora
- Datasheet-Pallet Scanning SystemDocumento3 pagineDatasheet-Pallet Scanning SystemSergio Tarancón GabásNessuna valutazione finora
- Manok Mabuhay (FINAL PAIR CASE)Documento12 pagineManok Mabuhay (FINAL PAIR CASE)Eldon CalambaNessuna valutazione finora
- Banking & Finance IndustryDocumento3 pagineBanking & Finance IndustryHrithik SaxenaNessuna valutazione finora
- Passengers' Perspective of Philippine Airlines Within Nueva EcijaDocumento15 paginePassengers' Perspective of Philippine Airlines Within Nueva EcijaPoonam KilaniyaNessuna valutazione finora
- City Union Bank Inspection ReportDocumento114 pagineCity Union Bank Inspection ReportMoneylife Foundation100% (1)
- Abhilesh SipDocumento42 pagineAbhilesh SiprahadipayanNessuna valutazione finora
- Ancient Greece - Unit PlanDocumento7 pagineAncient Greece - Unit PlanCosti TsakNessuna valutazione finora
- Mind Management Human Values BookDocumento94 pagineMind Management Human Values BookDhawal AgrawalNessuna valutazione finora
- Beta12CX Med Vented Cabinet High SPL Mid/High MonitorDocumento10 pagineBeta12CX Med Vented Cabinet High SPL Mid/High MonitorMarius GligorNessuna valutazione finora
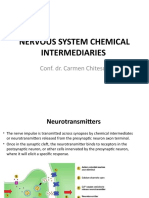
- NERVOUS SYSTEM CHEMICAL INTERMEDIARIESDocumento40 pagineNERVOUS SYSTEM CHEMICAL INTERMEDIARIESPopa NicuNessuna valutazione finora
- Emerging Markets Case Studies (ISSN: 2045-0621) Guide To Writing A Teaching Note Purpose of A Teaching NoteDocumento6 pagineEmerging Markets Case Studies (ISSN: 2045-0621) Guide To Writing A Teaching Note Purpose of A Teaching NoteFildzah FichanNessuna valutazione finora
- Creative Nonfiction Week 2 FINALDocumento12 pagineCreative Nonfiction Week 2 FINALFritzie SulitanaNessuna valutazione finora
- Flange Heaters - CX: Application CorrosionDocumento12 pagineFlange Heaters - CX: Application CorrosionGustav MolMedNessuna valutazione finora
- Formulation and Testing of Herbal Syrup For Cough and AsthmaDocumento11 pagineFormulation and Testing of Herbal Syrup For Cough and Asthmanaomiesolefack03Nessuna valutazione finora
- Kaiser-Meyer-Olkin Measure of Sampling Adequacy. .545 Bartlett's Test of Sphericity Approx. Chi-Square 199.860 DF 91 Sig. .000Documento4 pagineKaiser-Meyer-Olkin Measure of Sampling Adequacy. .545 Bartlett's Test of Sphericity Approx. Chi-Square 199.860 DF 91 Sig. .000Harpreet ThindNessuna valutazione finora
- Sense OrgansDocumento12 pagineSense OrgansRon GruellaNessuna valutazione finora
- Inorganic Chemistry Principles of Structure and Re Activity John Huheey 4th EditionDocumento1.049 pagineInorganic Chemistry Principles of Structure and Re Activity John Huheey 4th Editionluminary_iitbhu89% (65)
- GRADE 7 Third PT DivisionDocumento4 pagineGRADE 7 Third PT DivisionKingGamer 4595100% (1)
- Pfaff Tiptronic 1029Documento40 paginePfaff Tiptronic 1029Juhász MariannNessuna valutazione finora
- Module 3 - Topic 3Documento4 pagineModule 3 - Topic 3Moon LightNessuna valutazione finora
- 6 Rules For Teaching GrammarDocumento2 pagine6 Rules For Teaching GrammarBilly De Guzman Uson50% (2)
- Valuation of Goodwill: (1) Few Years' Purchase of Average Profits Method: Under ThisDocumento5 pagineValuation of Goodwill: (1) Few Years' Purchase of Average Profits Method: Under Thisabhi_cool7864757Nessuna valutazione finora
- Writing A Minutes of MeetingDocumento7 pagineWriting A Minutes of Meetingpreiquency100% (3)
- Eastside MasterplanDocumento23 pagineEastside MasterplanppinskiNessuna valutazione finora
- Models HL300 & HL400 ML-134351 ML-134348: 701 S. RIDGE AVENUE TROY, OHIO 45374-0001Documento24 pagineModels HL300 & HL400 ML-134351 ML-134348: 701 S. RIDGE AVENUE TROY, OHIO 45374-0001ZackyExlipzNessuna valutazione finora
- Basell PP Homo Rafia Hp456j Mi 3 4Documento2 pagineBasell PP Homo Rafia Hp456j Mi 3 4crawn06Nessuna valutazione finora
- Alcoa Wheel Service Manual For Trucks, Trailers, and BusesDocumento47 pagineAlcoa Wheel Service Manual For Trucks, Trailers, and BusesJenner Volnney Quispe ChataNessuna valutazione finora
- Data Structures Power Point PresentationDocumento54 pagineData Structures Power Point PresentationShreehari KulkarniNessuna valutazione finora