Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- DR Sonam's High Yield Notes For ST 2 & 5 2nd EditionDocumento251 pagineDR Sonam's High Yield Notes For ST 2 & 5 2nd EditionMuhammad Fahad100% (1)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- CNOR Free Practice Quiz - Zander Perioperative EducationDocumento13 pagineCNOR Free Practice Quiz - Zander Perioperative EducationJohnson100% (1)
- Test Bank For Personality and Personal Growth 7th Edition by FragerDocumento9 pagineTest Bank For Personality and Personal Growth 7th Edition by Fragera435418017Nessuna valutazione finora
- Steps in EndorsementDocumento7 pagineSteps in EndorsementGideon P. Casas100% (2)
- MbcmanualDocumento113 pagineMbcmanualapi-376080864Nessuna valutazione finora
- Chapter 21 Antidepressant AgentsDocumento4 pagineChapter 21 Antidepressant AgentsNicolle Lisay IlaganNessuna valutazione finora
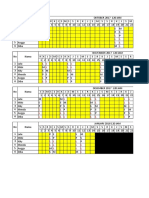
- Jadwal Baksos IshipDocumento5 pagineJadwal Baksos IshipFaradiba FebrianiNessuna valutazione finora
- Wrap Up Skenario 3 Blok Emergensi "Reaksi Obat": Kelompok A3Documento1 paginaWrap Up Skenario 3 Blok Emergensi "Reaksi Obat": Kelompok A3Faradiba FebrianiNessuna valutazione finora
- Wrap Up Skenario 1 Blok Medikolegal "Mata Diobati Menjadi Buta"Documento1 paginaWrap Up Skenario 1 Blok Medikolegal "Mata Diobati Menjadi Buta"Faradiba FebrianiNessuna valutazione finora
- The Agenda Comparative Study Students Representative Board Medical Faculty Yarsi UniversityDocumento1 paginaThe Agenda Comparative Study Students Representative Board Medical Faculty Yarsi UniversityFaradiba FebrianiNessuna valutazione finora
- EBM Critical AppraisalDocumento9 pagineEBM Critical AppraisalFaradiba FebrianiNessuna valutazione finora
- Sensory Physiology The Eye1Documento37 pagineSensory Physiology The Eye1Faradiba FebrianiNessuna valutazione finora
- Poisoning and ManagementDocumento53 paginePoisoning and ManagementYusuf Nawaz KhanNessuna valutazione finora
- Operating Room: Ns. Heri Kristianto. Skep., Mkep Department of Medical Surgical NursingDocumento21 pagineOperating Room: Ns. Heri Kristianto. Skep., Mkep Department of Medical Surgical NursingNizZa TakaricoNessuna valutazione finora
- Ganglion of The Hand and WristDocumento13 pagineGanglion of The Hand and WristtantraNessuna valutazione finora
- Infant and Young Child FeedingDocumento5 pagineInfant and Young Child FeedingRinjaya TeguhNessuna valutazione finora
- HCVDDocumento5 pagineHCVDkhrizaleehNessuna valutazione finora
- "My Neck Feels Stiff and There's Pain Coming From It. Every Time I Move It, It Only Gets Worse." As Stated by TheDocumento4 pagine"My Neck Feels Stiff and There's Pain Coming From It. Every Time I Move It, It Only Gets Worse." As Stated by TheCassey CuregNessuna valutazione finora
- Early OrthodonticsDocumento43 pagineEarly Orthodonticsdentistpro.org100% (1)
- Dialectical Behavior Therapy For Managing Interpersonal RelationshipsDocumento12 pagineDialectical Behavior Therapy For Managing Interpersonal RelationshipsJuan Alberto GonzálezNessuna valutazione finora
- CHARM Alt TrialDocumento5 pagineCHARM Alt TrialCristian Villarroel SNessuna valutazione finora
- Usepa 2014Documento16 pagineUsepa 2014walidNessuna valutazione finora
- Learning ContractDocumento2 pagineLearning Contractapi-285282702Nessuna valutazione finora
- MeningitisDocumento23 pagineMeningitisPutri RamadhaniNessuna valutazione finora
- BIANNUAL CONGRESS OF HOMOEOPATHIC ASSOCIATION OF SOUTH AFRICA (HSA) 2014: A REPORT (Prepared From REPORT: HSA CONGRESS 2014Documento6 pagineBIANNUAL CONGRESS OF HOMOEOPATHIC ASSOCIATION OF SOUTH AFRICA (HSA) 2014: A REPORT (Prepared From REPORT: HSA CONGRESS 2014Homoeopathic PulseNessuna valutazione finora
- Swog 8794Documento7 pagineSwog 8794yingming zhuNessuna valutazione finora
- Work Life Balance-NovartisDocumento86 pagineWork Life Balance-NovartisPurnima Puri100% (1)
- Treatment of Neglected Syndesmotic InjuriesDocumento16 pagineTreatment of Neglected Syndesmotic InjuriesMohamed GoudaNessuna valutazione finora
- Alzheimer's Disease: Its Homeopathic Management: Prokash MollickDocumento2 pagineAlzheimer's Disease: Its Homeopathic Management: Prokash MollickEnzoNessuna valutazione finora
- Abdominal ParacentesisDocumento31 pagineAbdominal Paracentesisbala kumaaranNessuna valutazione finora
- Breast AssesementDocumento18 pagineBreast AssesementDevy IselaNessuna valutazione finora
- Herbal Ectoparasiticidal DrugsDocumento0 pagineHerbal Ectoparasiticidal DrugsChai YawatNessuna valutazione finora
- Instant Download Ebook PDF Abnormal Psychology 6th Canadian Edition PDF ScribdDocumento41 pagineInstant Download Ebook PDF Abnormal Psychology 6th Canadian Edition PDF Scribdvictor.lewis791100% (40)
- Perawatan Saluran Akar Pada Sisa Akar Gigi Dengan Restorasi DirekDocumento7 paginePerawatan Saluran Akar Pada Sisa Akar Gigi Dengan Restorasi DirekNindya TamayaNessuna valutazione finora
- 6.principle of HDDocumento24 pagine6.principle of HDCaerulus Fuad Abdul BaqiNessuna valutazione finora
- Drug Study NurseryDocumento6 pagineDrug Study NurseryPau-pau BasiNessuna valutazione finora