Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- 1 Model General ConsimtamantDocumento15 pagine1 Model General Consimtamantcioaca12Nessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Cerere de Inregistrare Mentiuni Forme de ExercitareDocumento1 paginaCerere de Inregistrare Mentiuni Forme de Exercitarecioaca12Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Exercitiu ConflictDocumento2 pagineExercitiu Conflictcioaca12Nessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Model Telecomanda PDFDocumento12 pagineModel Telecomanda PDFcioaca12Nessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Fursecuri Nuci: IngredienteDocumento1 paginaFursecuri Nuci: Ingredientecioaca12Nessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- SDQ ScoringDocumento2 pagineSDQ Scoringcioaca120% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Lista Si ScorareDocumento1 paginaLista Si Scorarecioaca12Nessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Clinical Case Studies 2007 Townend 443 53Documento12 pagineClinical Case Studies 2007 Townend 443 53cioaca12Nessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Catalogue v09Documento4 pagineCatalogue v09KRISHNA L BAISETTINessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Dr. Dian Kusumaningrum - PRESENTASI JCCA-ANTIBIOTIC DOSING IN CRITICALLY ILLDocumento31 pagineDr. Dian Kusumaningrum - PRESENTASI JCCA-ANTIBIOTIC DOSING IN CRITICALLY ILLRestu TriwulandaniNessuna valutazione finora
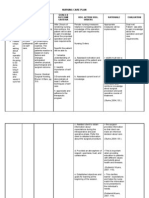
- Sample Nurses Notes CuDocumento3 pagineSample Nurses Notes Cuapi-1978086589% (19)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Sleep Apnea Research PaperDocumento9 pagineSleep Apnea Research Paperaflbuagdw100% (3)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- PhilippinesDocumento9 paginePhilippinesIvy Geraldine FerrerNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Principles Involved in Bioassay by Different Methods A Minireview PDFDocumento18 paginePrinciples Involved in Bioassay by Different Methods A Minireview PDFPankaj KushwahNessuna valutazione finora
- NCP 1Documento4 pagineNCP 1Ke EjieNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Jpoa 2023 Feb PDFDocumento163 pagineJpoa 2023 Feb PDFOscar MontilvaNessuna valutazione finora
- Rumah Sakit Bhakti MuliaDocumento3 pagineRumah Sakit Bhakti MuliaSarachanda SallyNessuna valutazione finora
- Cancer Pathophysiology FinalDocumento3 pagineCancer Pathophysiology FinalAngelique Ramos Pascua100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Dayan Aka Wild-Goose - Qigong IntroducionDocumento2 pagineDayan Aka Wild-Goose - Qigong IntroducionTest4D100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Chest Tube DrainageDocumento4 pagineChest Tube DrainageJoshua Andre PepitoNessuna valutazione finora
- Modalitas RehabmedikDocumento115 pagineModalitas RehabmedikWegrimel AriegaraNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- PMLS Lesson 4Documento3 paginePMLS Lesson 4Void MelromarcNessuna valutazione finora
- Detoxification Therapeutics For Heavy Metals, Toxic Chemicals and Other NeurotoxinsDocumento175 pagineDetoxification Therapeutics For Heavy Metals, Toxic Chemicals and Other Neurotoxins300r100% (9)
- Philhealth Cf4 2017-2018Documento8 paginePhilhealth Cf4 2017-2018Julius Yves Dulfo BagacayNessuna valutazione finora
- Hypertension Management: Key RecommendationsDocumento76 pagineHypertension Management: Key RecommendationsPritam DugarNessuna valutazione finora
- Labs and Impaired Tissue...Documento40 pagineLabs and Impaired Tissue...Lea FestejoNessuna valutazione finora
- Kidney TransplantationDocumento5 pagineKidney TransplantationDeadly ChillerNessuna valutazione finora
- Stugeron ForteDocumento4 pagineStugeron ForteJemsMei Comparativo MensuradoNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Adult and Elder I. Nursing Care PlanDocumento6 pagineAdult and Elder I. Nursing Care PlanteresapazNessuna valutazione finora
- Guidebook For Preacc Entrylevelstandards SHCO PDFDocumento162 pagineGuidebook For Preacc Entrylevelstandards SHCO PDFArun Kumar100% (3)
- Ethics and Patient SafetyDocumento10 pagineEthics and Patient SafetyIdeas InfiniteNessuna valutazione finora
- Who Trs 908 Informe 37 Part10Documento14 pagineWho Trs 908 Informe 37 Part10dani20153Nessuna valutazione finora
- In Vitro in Vivo Correlation Ivivc A Strategic Tool in Drug Development Jbb.S3 001Documento12 pagineIn Vitro in Vivo Correlation Ivivc A Strategic Tool in Drug Development Jbb.S3 001Jerome K GeorgeNessuna valutazione finora
- FINAL EXAM-SY 2020-2021 NCM-117: Fides Et ServitiumDocumento7 pagineFINAL EXAM-SY 2020-2021 NCM-117: Fides Et ServitiumDatujen SanayatinNessuna valutazione finora
- Water Treatment Plant Residue Management ModificationDocumento33 pagineWater Treatment Plant Residue Management ModificationNitisha Rathore50% (2)
- Mindful Medical Practice - Clinical Narratives and Therapeutic InsightsDocumento169 pagineMindful Medical Practice - Clinical Narratives and Therapeutic InsightsSkg KonNessuna valutazione finora
- Amit Tracheostomy Presentation 12 Aug 2010Documento59 pagineAmit Tracheostomy Presentation 12 Aug 2010Amit KochetaNessuna valutazione finora
- Acceptance and Mindfulness Treatments For Children and Adolescents. A Practitioner's Guide - Greco, L. y Hayes, S.Documento249 pagineAcceptance and Mindfulness Treatments For Children and Adolescents. A Practitioner's Guide - Greco, L. y Hayes, S.Antonella María De Jesús Napán Carbajal100% (4)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)