Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Pediatric Physical Assessment With AudioDocumento47 paginePediatric Physical Assessment With AudioKathleen Montaño100% (1)
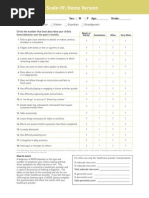
- Screening ADHDDocumento2 pagineScreening ADHDPsiholog Alina Mirela CraiuNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- HIRA For Loading or Unloading ActivityDocumento4 pagineHIRA For Loading or Unloading ActivityMD Abdullah100% (2)
- Usmle Essential BooksDocumento3 pagineUsmle Essential BooksBhavin Choksi33% (3)
- Nursing Board Review Medical SurgicalDocumento9 pagineNursing Board Review Medical SurgicalPhilip Simangan0% (1)
- PneumoniaDocumento17 paginePneumoniajustin_saneNessuna valutazione finora
- Frcs General Surgery Mcqs Pdfsdocuments2comwwwpdfsdocuments2comf54frcs General Surgery MCQSPDFPDFDocumento2 pagineFrcs General Surgery Mcqs Pdfsdocuments2comwwwpdfsdocuments2comf54frcs General Surgery MCQSPDFPDFAbbas Ali0% (1)
- Tle10 - Afa - Animalprodpoultry - q2 - Mod9 - Performingpreventive - Treatmentmeasures (1) - v3 (66 Pages)Documento67 pagineTle10 - Afa - Animalprodpoultry - q2 - Mod9 - Performingpreventive - Treatmentmeasures (1) - v3 (66 Pages)Erwin Poblete AraraoNessuna valutazione finora
- Breast Calcification - A Diagnostic ManualDocumento209 pagineBreast Calcification - A Diagnostic ManualGrace Georgina Saldana100% (3)
- Nuevo Curriculo Ingles 2017Documento92 pagineNuevo Curriculo Ingles 2017Joe Felipe Vera OchoaNessuna valutazione finora
- Cirrosis Biliar Primaria Fisiopatología Presentación Clínica y La TerapiaDocumento17 pagineCirrosis Biliar Primaria Fisiopatología Presentación Clínica y La TerapiaJoe Felipe Vera OchoaNessuna valutazione finora
- Case 31-2016 A 53-Year-Old ManDocumento12 pagineCase 31-2016 A 53-Year-Old ManJoe Felipe Vera OchoaNessuna valutazione finora
- Ascorbic Acid PEG-2L Is Superior For Early MorningDocumento9 pagineAscorbic Acid PEG-2L Is Superior For Early MorningJoe Felipe Vera OchoaNessuna valutazione finora
- Cambios en El Diagnostico de Hepatitis C-Jama 2014Documento2 pagineCambios en El Diagnostico de Hepatitis C-Jama 2014Joe Felipe Vera OchoaNessuna valutazione finora
- G2 CHAPTER 2finalDocumento15 pagineG2 CHAPTER 2finalMike AntolinoNessuna valutazione finora
- Aspek Etik Dan Legal Dalam Keperawatan BencanaDocumento11 pagineAspek Etik Dan Legal Dalam Keperawatan BencanaPhiioNessuna valutazione finora
- Ethiopia Food-Based Dietary Guidelines 2022Documento108 pagineEthiopia Food-Based Dietary Guidelines 2022Melka Girma100% (2)
- HIV/AIDS Education GuideDocumento12 pagineHIV/AIDS Education GuideDutch EarthNessuna valutazione finora
- Cross Sectional Studies Hemed 2015Documento12 pagineCross Sectional Studies Hemed 2015delovinaNessuna valutazione finora
- Mo2vate Issue 15 - March 2022Documento74 pagineMo2vate Issue 15 - March 2022Mo2vate MagazineNessuna valutazione finora
- Fenner Handbook 2011Documento55 pagineFenner Handbook 2011Mehdi AlizadehNessuna valutazione finora
- Coronavirus (COVID-19) RecordsDocumento1 paginaCoronavirus (COVID-19) RecordsMarium BhalaNessuna valutazione finora
- All India Network Hospitals GeneralDocumento630 pagineAll India Network Hospitals GeneralPankajNessuna valutazione finora
- Medical Treatment Recuperation Convalescence With HomoeopathyDocumento4 pagineMedical Treatment Recuperation Convalescence With HomoeopathyEditor IJTSRDNessuna valutazione finora
- PPT Referat Syok Argia AnjaniDocumento34 paginePPT Referat Syok Argia Anjanidhana2395Nessuna valutazione finora
- The Social Norms ApproachDocumento7 pagineThe Social Norms ApproachJasmine TereaNessuna valutazione finora
- FluidDocumento190 pagineFluidAndrias OzNessuna valutazione finora
- Doh NOTES-1Documento196 pagineDoh NOTES-1norabilbaoNessuna valutazione finora
- Hivaids Related Knowledge Attitude Risk Perception and Sexual BehaviorDocumento5 pagineHivaids Related Knowledge Attitude Risk Perception and Sexual BehaviorIJARP PublicationsNessuna valutazione finora
- Drexel University: Commencement Ceremonies College of MedicineDocumento25 pagineDrexel University: Commencement Ceremonies College of MedicineChimpNessuna valutazione finora
- Nursing PresentationDocumento63 pagineNursing PresentationDeekayNessuna valutazione finora
- Define 1. EntrepreneurialDocumento8 pagineDefine 1. EntrepreneurialJake Yvan DizonNessuna valutazione finora
- Reflection 1Documento5 pagineReflection 1api-400554289Nessuna valutazione finora
- Why To Not Legalize EuthanasiaDocumento5 pagineWhy To Not Legalize EuthanasiaScotiaccap2016Nessuna valutazione finora
- How Many Implants Are Necessary To Stabilise An Implant-Supported Maxillary Overdenture?Documento2 pagineHow Many Implants Are Necessary To Stabilise An Implant-Supported Maxillary Overdenture?Erick Brañes EspinozaNessuna valutazione finora