Potrebbero piacerti anche
- Next Generation Sequencing of Microbial Cell Free DNA To Rapidly Detect Fluoribacter Bozemanae Pneumonia in An Immunocompromised HostDocumento4 pagineNext Generation Sequencing of Microbial Cell Free DNA To Rapidly Detect Fluoribacter Bozemanae Pneumonia in An Immunocompromised HostAthenaeum Scientific PublishersNessuna valutazione finora
- Jurnal 2Documento16 pagineJurnal 2grace liwantoNessuna valutazione finora
- Leptospirosis Diagnosis: Competancy of Various Laboratory TestsDocumento18 pagineLeptospirosis Diagnosis: Competancy of Various Laboratory TestsAnonymous Dj9d9MNessuna valutazione finora
- LEPTOSPIROSISDocumento4 pagineLEPTOSPIROSISMartin TanNessuna valutazione finora
- Current Status of Leprosy: Epidemiology, Basic Science and Clinical PerspectivesDocumento9 pagineCurrent Status of Leprosy: Epidemiology, Basic Science and Clinical PerspectivesYolan Sentika NovaldiNessuna valutazione finora
- Microorganisms 07 00179 With CoverDocumento18 pagineMicroorganisms 07 00179 With CoverBenga TokanneNessuna valutazione finora
- Gonorrhoea in Men: Diagnostic Aspects and Changing Antibiotic Susceptibility PatternDocumento4 pagineGonorrhoea in Men: Diagnostic Aspects and Changing Antibiotic Susceptibility PatternAlthaf FathanNessuna valutazione finora
- 1 s2.0 S1201971214015732 MainDocumento18 pagine1 s2.0 S1201971214015732 MainMichael JonesNessuna valutazione finora
- A Fast and Highly Sensitive Blood Culture PCR For SalmonellaDocumento7 pagineA Fast and Highly Sensitive Blood Culture PCR For SalmonellaMd. Tanjil IslamNessuna valutazione finora
- Malaria PDFDocumento17 pagineMalaria PDFPrizzie PotosíNessuna valutazione finora
- Tropicalmed 07 00260Documento21 pagineTropicalmed 07 00260فرجني موغNessuna valutazione finora
- Evaluation of qPCR-Based Assays For Leprosy Diagnosis Directly in Clinical SpecimensDocumento8 pagineEvaluation of qPCR-Based Assays For Leprosy Diagnosis Directly in Clinical SpecimenszemanesilvaNessuna valutazione finora
- Laboratory Diagnosis of Leptospirosis: A Challenge: Didier Musso, Bernard La ScolaDocumento8 pagineLaboratory Diagnosis of Leptospirosis: A Challenge: Didier Musso, Bernard La ScolaAnna Diaz YuberoNessuna valutazione finora
- Jurnal Tifoid C 2Documento12 pagineJurnal Tifoid C 2Yulia PuspitaNessuna valutazione finora
- Clinmed-22-1-14 Linical AspectsDocumento4 pagineClinmed-22-1-14 Linical AspectsSara Valentina GarciaNessuna valutazione finora
- Adilistya 2020Documento1 paginaAdilistya 2020shahhareshNessuna valutazione finora
- Diagnosis of TuberculosisDocumento62 pagineDiagnosis of TuberculosisEshani DewanNessuna valutazione finora
- DETEKSI TBDocumento7 pagineDETEKSI TBSetiaty PandiaNessuna valutazione finora
- Islam S, Rahman F, Saurab K M, Ahmed J, Kamal SMM, Noor RDocumento9 pagineIslam S, Rahman F, Saurab K M, Ahmed J, Kamal SMM, Noor RLUIS ALBERTO DE LA HOZ BARRIENTOSNessuna valutazione finora
- Thesis Jessica KattanDocumento45 pagineThesis Jessica Kattanaztigan100% (2)
- JP 05073Documento6 pagineJP 05073Link BuiNessuna valutazione finora
- Review 01-06 PDFDocumento6 pagineReview 01-06 PDFEditor IjprtNessuna valutazione finora
- Evaluation of Real-Time PCR and Culturing For The Detection of Leptospires in Canine SamplesDocumento9 pagineEvaluation of Real-Time PCR and Culturing For The Detection of Leptospires in Canine SamplesraviggNessuna valutazione finora
- Abordaje Linfadenopatia PerifericaDocumento13 pagineAbordaje Linfadenopatia PerifericaTony Gomez Luna LeyvaNessuna valutazione finora
- 2.3 Intestinal ParasitesDocumento2 pagine2.3 Intestinal ParasitesDiego CushicóndorNessuna valutazione finora
- Deteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Documento8 pagineDeteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Anonymous iJc2y0Nessuna valutazione finora
- Fite - FaracoDocumento8 pagineFite - Faracoirwan junNessuna valutazione finora
- Jurnal Kusta PDFDocumento13 pagineJurnal Kusta PDFGustamas Indra Maulana100% (1)
- Different Diagnostic Procedure of Typhoid Fever ADocumento8 pagineDifferent Diagnostic Procedure of Typhoid Fever AdjebrutNessuna valutazione finora
- LeprosyDocumento6 pagineLeprosyAna Delia LabianoNessuna valutazione finora
- Annals of Clinical Microbiology and AntimicrobialsDocumento10 pagineAnnals of Clinical Microbiology and AntimicrobialsWadramys SoumsNessuna valutazione finora
- Lepto 1Documento15 pagineLepto 1Achmad Sya'idNessuna valutazione finora
- Medical Microbiology Course on Spirochetes and NeisseriaDocumento4 pagineMedical Microbiology Course on Spirochetes and NeisseriaMuneer Al-DahbaliNessuna valutazione finora
- Leptospirosis Guide: Causes, Symptoms and TreatmentDocumento6 pagineLeptospirosis Guide: Causes, Symptoms and TreatmentalvinbbNessuna valutazione finora
- Laboratory Diagnosis of Infectious Diseases GuidelineDocumento100 pagineLaboratory Diagnosis of Infectious Diseases GuidelineGalo PinosNessuna valutazione finora
- Jurnal 2Documento9 pagineJurnal 2Rio ArdiantoruNessuna valutazione finora
- A Quantitative PCR (Taqman) Assay For Pathogenic: Leptospira SPPDocumento22 pagineA Quantitative PCR (Taqman) Assay For Pathogenic: Leptospira SPPVigneshwaran RavishankarNessuna valutazione finora
- A Review On Epidemiology, Pathogenesis and Treatment of LeptospirosisDocumento7 pagineA Review On Epidemiology, Pathogenesis and Treatment of LeptospirosisIJAR JOURNALNessuna valutazione finora
- Diagnosis of MalariaDocumento15 pagineDiagnosis of MalariaSuranjan Pal100% (1)
- 4788 ID Faktor Risiko Lingkungan Kejadian Leptospirosis Di Jawa Tengah Studi Kasus Di Ko PDFDocumento8 pagine4788 ID Faktor Risiko Lingkungan Kejadian Leptospirosis Di Jawa Tengah Studi Kasus Di Ko PDFbintang nurzakiahNessuna valutazione finora
- LeptospirosisDocumento8 pagineLeptospirosisSanda Puspa RiniNessuna valutazione finora
- Penicillium Marneffei Infection in HIV/AIDS PatientsDocumento33 paginePenicillium Marneffei Infection in HIV/AIDS PatientsNaman Kongari0% (1)
- LeptospirosisDocumento14 pagineLeptospirosisClement ThansNessuna valutazione finora
- PCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative PathogensDocumento7 paginePCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative Pathogensfaraz.mirza1Nessuna valutazione finora
- Diagnostic VirologyDocumento46 pagineDiagnostic VirologySarah DadoNessuna valutazione finora
- Legionnaires' Disease Seminar ReviewDocumento10 pagineLegionnaires' Disease Seminar Reviewcrowned-lionNessuna valutazione finora
- TB JournalDocumento1 paginaTB JournalJudy Anne PatricioNessuna valutazione finora
- Pathogens 12 00135Documento12 paginePathogens 12 00135Isa Andrea Aro TarquiNessuna valutazione finora
- Neonatal fungal infections diagnosis strategiesDocumento4 pagineNeonatal fungal infections diagnosis strategiesirdinamarchsyaNessuna valutazione finora
- Arch Dis Child 1998 Ladhani 85 8Documento5 pagineArch Dis Child 1998 Ladhani 85 8Dian Ayu Permata SandiNessuna valutazione finora
- Amebiasis: Aspectos Clínicos, Terapéuticos y de Diagnóstico de La InfecciónDocumento8 pagineAmebiasis: Aspectos Clínicos, Terapéuticos y de Diagnóstico de La Infección2022110046 HERNANDO JOSE DIAZ GONZALEZ ESTUDIANTE ACTIVONessuna valutazione finora
- Morphological Features and Differential Counts of Plasmodium Knowlesi Parasites in Naturally Acquired Human InfectionsDocumento10 pagineMorphological Features and Differential Counts of Plasmodium Knowlesi Parasites in Naturally Acquired Human InfectionsAnantaBenvenutoNessuna valutazione finora
- MALÁRIA No Celldyn TrabalhoDocumento5 pagineMALÁRIA No Celldyn TrabalhoAlexandre MedeirosNessuna valutazione finora
- Clinmed 22 1 14Documento4 pagineClinmed 22 1 14Familia CarbajalNessuna valutazione finora
- Etiology: Leptospira Are Aerobic, Gram-Negative Spirochetes That Are Fastidious, Slow Growing, and HaveDocumento9 pagineEtiology: Leptospira Are Aerobic, Gram-Negative Spirochetes That Are Fastidious, Slow Growing, and HaveIulia_Julee_4578Nessuna valutazione finora
- 5 Metode Eksperimen Dna 13 Oktober 2022Documento7 pagine5 Metode Eksperimen Dna 13 Oktober 2022debiNessuna valutazione finora
- Toxoplasmosis: New Challenges For An Old DiseaseDocumento5 pagineToxoplasmosis: New Challenges For An Old DiseaseNovi Alviani KamalNessuna valutazione finora
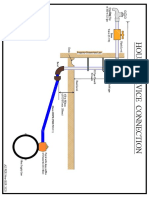
- House Service Connection NEW BSR 2020-1Documento1 paginaHouse Service Connection NEW BSR 2020-1Deshraj BairwaNessuna valutazione finora
- CH 2 Atoms, Ions, and MoleculesDocumento64 pagineCH 2 Atoms, Ions, and MoleculesBritney SimmsNessuna valutazione finora
- Finger Print Based Voting System For Rigging Free Governing SystemDocumento2 pagineFinger Print Based Voting System For Rigging Free Governing SystemArvind TilotiaNessuna valutazione finora
- DD Cen TR 10347-2006Documento14 pagineDD Cen TR 10347-2006prabagaran88% (8)
- GadDocumento1 paginaGadFakhruddin DhilawalaNessuna valutazione finora
- Captain Marvel (DC Comics) : Shazam! Navigation SearchDocumento34 pagineCaptain Marvel (DC Comics) : Shazam! Navigation SearchAce Orense Cupid Uranus Ace Sphinx Galzu Acetr444 son of Multiverses Chaos Gaeia Eros ACETR444Nessuna valutazione finora
- E5971 m4n68t-m Series ManualDocumento0 pagineE5971 m4n68t-m Series ManualcamiloelosadaNessuna valutazione finora
- The Effects of Oar-Shaft Stiffness andDocumento9 pagineThe Effects of Oar-Shaft Stiffness andValentina DiamanteNessuna valutazione finora
- W2AEW Videos (Apr 29, 2017) Topics Listed NumericallyDocumento12 pagineW2AEW Videos (Apr 29, 2017) Topics Listed Numericallyamol1agarwalNessuna valutazione finora
- Overview of US Investment in NanotechnologyDocumento19 pagineOverview of US Investment in NanotechnologyMaterials Research InstituteNessuna valutazione finora
- Megger FORMDocumento1 paginaMegger FORMCOSMOPOLITAN M&ENessuna valutazione finora
- Qanooneislamorcu 00 JafaDocumento646 pagineQanooneislamorcu 00 JafaawNessuna valutazione finora
- Error Codes (DTC) : 15 Electrical TroubleshootingDocumento13 pagineError Codes (DTC) : 15 Electrical TroubleshootingPoyraz PoyrazNessuna valutazione finora
- Simple LED Flasher CircuitsDocumento5 pagineSimple LED Flasher CircuitsVivek BNessuna valutazione finora
- MSE Admission and Degree RequirementsDocumento6 pagineMSE Admission and Degree Requirementsdeathbuddy_87Nessuna valutazione finora
- AmadeusDocumento3 pagineAmadeusCleofe Mae Piñero AseñasNessuna valutazione finora
- Geneaid DNA Reagent Plant GR200Documento4 pagineGeneaid DNA Reagent Plant GR200Gandi SogandiNessuna valutazione finora
- IOM Paquetes DX Precedent RT-SVX22U-EN - 03072018Documento82 pagineIOM Paquetes DX Precedent RT-SVX22U-EN - 03072018Mario Lozano100% (1)
- CQ B TECHNIQUESDocumento37 pagineCQ B TECHNIQUESeddie6355100% (3)
- Price List Grand I10 Nios DT 01.05.2022Documento1 paginaPrice List Grand I10 Nios DT 01.05.2022VijayNessuna valutazione finora
- Common Sense Renewed R. C. ChristianDocumento276 pagineCommon Sense Renewed R. C. Christianwarhed76100% (3)
- Curriculum Map Science 8 2023 2024Documento12 pagineCurriculum Map Science 8 2023 2024Gehan Lorefel Durante TibayNessuna valutazione finora
- 13.phase Feeding and Feeding SystemsDocumento21 pagine13.phase Feeding and Feeding SystemsAsfand Ali SheikhNessuna valutazione finora
- 3ixso2idq334tonwmfhk0rrcDocumento2 pagine3ixso2idq334tonwmfhk0rrcrishikeshraj2021Nessuna valutazione finora
- Potensi Energi Listrik Yang Dihasilkan Dari Emisi Gas Metana Di Tpa Suwung Provinsi BaliDocumento8 paginePotensi Energi Listrik Yang Dihasilkan Dari Emisi Gas Metana Di Tpa Suwung Provinsi BaliNuyul FaizahNessuna valutazione finora
- PWC Verbal Past Question and Answer 1Documento130 paginePWC Verbal Past Question and Answer 1Anton PermanaNessuna valutazione finora
- Danniel Martinez Gonzalez - Gizmo: Seasons: Earth, Moon and Sun Activity B Due 2.3 Deadline 3.1Documento3 pagineDanniel Martinez Gonzalez - Gizmo: Seasons: Earth, Moon and Sun Activity B Due 2.3 Deadline 3.1dannielNessuna valutazione finora
- Countable UncountableDocumento4 pagineCountable UncountablePaoLo Mena la TorreNessuna valutazione finora
- Self EducationDocumento21 pagineSelf EducationSwami VedatitanandaNessuna valutazione finora
- Sektion Installation Guide Fy21 Web ADocumento16 pagineSektion Installation Guide Fy21 Web AmroliverridleyNessuna valutazione finora