Potrebbero piacerti anche
- Ziopharm Slides To Accompany Q3 2019 Call 110719 FinalDocumento13 pagineZiopharm Slides To Accompany Q3 2019 Call 110719 FinalBLBVORTEXNessuna valutazione finora
- Blackrockgold Presentation July-3Documento26 pagineBlackrockgold Presentation July-3BLBVORTEXNessuna valutazione finora
- Global - Close To Peak USD LiquidityDocumento7 pagineGlobal - Close To Peak USD LiquidityBLBVORTEXNessuna valutazione finora
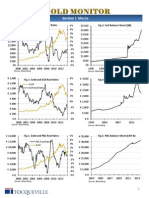
- Tocqueville Gold Monitor 4Q 2013Documento11 pagineTocqueville Gold Monitor 4Q 2013Gold Silver WorldsNessuna valutazione finora
- DVAX Coporate Presentation Strong Buy...Documento26 pagineDVAX Coporate Presentation Strong Buy...BLBVORTEXNessuna valutazione finora
- Sarepta JPM 2019 FinalDocumento26 pagineSarepta JPM 2019 FinalBLBVORTEXNessuna valutazione finora
- Fs SP 500 Utilities SectorDocumento6 pagineFs SP 500 Utilities SectorBLBVORTEXNessuna valutazione finora
- Oil Strategy - The Conviction ListDocumento23 pagineOil Strategy - The Conviction ListBLBVORTEXNessuna valutazione finora
- GloomBoomDoom Report Monetary TectonicsDocumento4 pagineGloomBoomDoom Report Monetary TectonicsBLBVORTEXNessuna valutazione finora
- CIMB Navigating Thailand 2015 Dec 2014 PDFDocumento212 pagineCIMB Navigating Thailand 2015 Dec 2014 PDFBLBVORTEXNessuna valutazione finora
- BIS Working Papers 2Documento35 pagineBIS Working Papers 2AdminAliNessuna valutazione finora
- Current Tanker RatesSept12Documento3 pagineCurrent Tanker RatesSept12BLBVORTEXNessuna valutazione finora
- Copper Mountain August 2014 Corp PresDocumento29 pagineCopper Mountain August 2014 Corp PresBLBVORTEXNessuna valutazione finora
- KPMG China Pharmaceutical 201106Documento62 pagineKPMG China Pharmaceutical 201106merc2Nessuna valutazione finora
- BTG Petrobras January 2015Documento7 pagineBTG Petrobras January 2015BLBVORTEXNessuna valutazione finora
- CAPR ARM Investor DayDocumento19 pagineCAPR ARM Investor DayBLBVORTEXNessuna valutazione finora
- VIPS 2Q13 Post Earnings PresentationDocumento28 pagineVIPS 2Q13 Post Earnings PresentationBLBVORTEXNessuna valutazione finora
- UBS Research Focus, Sustainable Investing, July 2013.Documento40 pagineUBS Research Focus, Sustainable Investing, July 2013.Glenn ViklundNessuna valutazione finora
- India Agriculture Inputs Seeds of Prosperity 26-02-14!15!05Documento87 pagineIndia Agriculture Inputs Seeds of Prosperity 26-02-14!15!05BLBVORTEX100% (1)
- Commodities Update - CIBC - Dec 2Documento8 pagineCommodities Update - CIBC - Dec 2BLBVORTEXNessuna valutazione finora
- Asia Pacific Equities Malaysia May 8th 2013Documento7 pagineAsia Pacific Equities Malaysia May 8th 2013BLBVORTEXNessuna valutazione finora
- OEl Gas LatAmDocumento76 pagineOEl Gas LatAmBLBVORTEXNessuna valutazione finora
- CLSA Greed Fear 1 August 2013Documento13 pagineCLSA Greed Fear 1 August 2013BLBVORTEXNessuna valutazione finora
- IndiapharmaDocumento151 pagineIndiapharmaBLBVORTEXNessuna valutazione finora
- Sucden Financial Quarterly Metals Report October 2013Documento60 pagineSucden Financial Quarterly Metals Report October 2013BLBVORTEXNessuna valutazione finora
- Greater China Smartphone Sector 130904Documento52 pagineGreater China Smartphone Sector 130904BLBVORTEXNessuna valutazione finora
- Occ Asional Paper Series: China'S Economic Growth and RebalancingDocumento56 pagineOcc Asional Paper Series: China'S Economic Growth and RebalancingRupojit RoyNessuna valutazione finora
- Strategy Bocom June 2013Documento6 pagineStrategy Bocom June 2013BLBVORTEXNessuna valutazione finora
- Philips Securities 2013 China Macroeconomic Semiannual Report 130726Documento5 paginePhilips Securities 2013 China Macroeconomic Semiannual Report 130726BLBVORTEXNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 02 Nasir Javaid PDFDocumento33 pagine02 Nasir Javaid PDFUmer DhillonNessuna valutazione finora
- MBA (Pharmaceutical Management) : Semester-1Documento23 pagineMBA (Pharmaceutical Management) : Semester-1HarshaNessuna valutazione finora
- 05langston Modern Meat: Synthetic Hormones, Livestock, and Consumers in The Post-WWII Era Nancy Langston UW-Madison Nelangst@wisc - EduDocumento34 pagine05langston Modern Meat: Synthetic Hormones, Livestock, and Consumers in The Post-WWII Era Nancy Langston UW-Madison Nelangst@wisc - EduSFLDNessuna valutazione finora
- Kratom Feasibility Report SupplementDocumento92 pagineKratom Feasibility Report SupplementMichael_Roberts2019Nessuna valutazione finora
- Press Release (Company Update)Documento3 paginePress Release (Company Update)Shyam SunderNessuna valutazione finora
- A Movement RisingDocumento22 pagineA Movement RisingDejan ŠešlijaNessuna valutazione finora
- Notice: Grant and Cooperative Agreement Awards: Community Development Work Study ProgramDocumento3 pagineNotice: Grant and Cooperative Agreement Awards: Community Development Work Study ProgramJustia.comNessuna valutazione finora
- Legal Aspects of Cosmetic Products: Development TeamDocumento24 pagineLegal Aspects of Cosmetic Products: Development TeamkashishNessuna valutazione finora
- Emperador 2013Documento114 pagineEmperador 2013collieNessuna valutazione finora
- NLM Pillbox API Documentation v2 2011.09.27Documento7 pagineNLM Pillbox API Documentation v2 2011.09.27Vignesh PTNessuna valutazione finora
- Rare Diseases 2013 PDFDocumento56 pagineRare Diseases 2013 PDFantikenomaNessuna valutazione finora
- Frauds and Deceptions Affecting The Elderly: Investigations, Findings, and RecommendationsDocumento94 pagineFrauds and Deceptions Affecting The Elderly: Investigations, Findings, and RecommendationsPetre ZamfirNessuna valutazione finora
- Thai Beverage Conference BrochureDocumento6 pagineThai Beverage Conference BrochurexinvtNessuna valutazione finora
- May 5, 2021: BioNTech's Cover Letter Re Application For Marketing of ComirnatyDocumento6 pagineMay 5, 2021: BioNTech's Cover Letter Re Application For Marketing of ComirnatyBrian O'SheaNessuna valutazione finora
- LGM Pharma - Active Pharmaceutical Ingredient SupplierDocumento11 pagineLGM Pharma - Active Pharmaceutical Ingredient SupplierLGM PharmaNessuna valutazione finora
- Business Ethics and Social ResponsibilityDocumento44 pagineBusiness Ethics and Social Responsibilitydinar aimcNessuna valutazione finora
- Regulatory Education for Industry (REdI): GENERIC DRUGS FORUM Dissolution Method Development PresentationDocumento17 pagineRegulatory Education for Industry (REdI): GENERIC DRUGS FORUM Dissolution Method Development PresentationAnnisaIndahPNessuna valutazione finora
- MelatoninDocumento22 pagineMelatoninVassily RubachofNessuna valutazione finora
- DOE Et Al v. AUSTIN Et Al, Case Number 3 - 21-Cv-01211, 12 NOV 21, US District Court For The Northern District of Florida, Pages 12-15.cleanedDocumento35 pagineDOE Et Al v. AUSTIN Et Al, Case Number 3 - 21-Cv-01211, 12 NOV 21, US District Court For The Northern District of Florida, Pages 12-15.cleanedAl Statilius100% (1)
- DOH NTFjao2021 0001Documento14 pagineDOH NTFjao2021 0001arhielleNessuna valutazione finora
- FDA Clinical Trial Requirements For Medical DevicesDocumento38 pagineFDA Clinical Trial Requirements For Medical DevicesUri HofferNessuna valutazione finora
- Kill Box PresentationDocumento18 pagineKill Box PresentationSerge BièvreNessuna valutazione finora
- Vera v. CuevasDocumento3 pagineVera v. CuevasJulia Alexandra ChuNessuna valutazione finora
- QAQC Medical DeviceDocumento32 pagineQAQC Medical DeviceMOHNISH MANCHALWARNessuna valutazione finora
- You Are Not Sick You Are ThirstyDocumento3 pagineYou Are Not Sick You Are ThirstyIgor Feitoza100% (1)
- Steven Zhang ResumeDocumento2 pagineSteven Zhang Resumeapi-534987967Nessuna valutazione finora
- WWW - Kfda.go - KR: Registration Number 11-1470000-001902-01Documento162 pagineWWW - Kfda.go - KR: Registration Number 11-1470000-001902-01yoganaNessuna valutazione finora
- Patient-focused Drug Development Incorporates Patient VoiceDocumento9 paginePatient-focused Drug Development Incorporates Patient Voicephoto copyhemnNessuna valutazione finora
- CREW: Department of Health and Human Services: Public Affairs Firms Documents: 01/24/07: HHS/FDA FOIA ResponseDocumento247 pagineCREW: Department of Health and Human Services: Public Affairs Firms Documents: 01/24/07: HHS/FDA FOIA ResponseCREWNessuna valutazione finora
- Abbott ABT PDFDocumento39 pagineAbbott ABT PDFuygh g100% (1)