Potrebbero piacerti anche
- 1Documento1 pagina1rachmyhamdiNessuna valutazione finora
- Psychiatric Bulletin 2014 Milward 144Documento3 paginePsychiatric Bulletin 2014 Milward 144rachmyhamdiNessuna valutazione finora
- Dunkel Schetter Tanner 2012 COPsychiatryDocumento8 pagineDunkel Schetter Tanner 2012 COPsychiatryrachmyhamdiNessuna valutazione finora
- Breech SungsangDocumento3 pagineBreech SungsangrachmyhamdiNessuna valutazione finora
- Bandelow - Et - Al - 01 Pharma Anxiety Disorders Primary CareDocumento8 pagineBandelow - Et - Al - 01 Pharma Anxiety Disorders Primary Carescabrera_scribdNessuna valutazione finora
- Temukan 1 Kata DickyDocumento11 pagineTemukan 1 Kata DickyrachmyhamdiNessuna valutazione finora
- Temukan 1 Kata DickyDocumento11 pagineTemukan 1 Kata DickyrachmyhamdiNessuna valutazione finora
- Temukan 1 Kata DickyDocumento11 pagineTemukan 1 Kata DickyrachmyhamdiNessuna valutazione finora
- Chapt 8Documento3 pagineChapt 8rachmyhamdiNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Those With MoonDocumento1 paginaThose With MoonRosee AldamaNessuna valutazione finora
- Basics of Fire SprinklerDocumento21 pagineBasics of Fire SprinklerLeo_1982Nessuna valutazione finora
- ISO - TR - 15608 - 2017 (En) - Pipe Grouping SystemsDocumento12 pagineISO - TR - 15608 - 2017 (En) - Pipe Grouping SystemsTeodor ProdanNessuna valutazione finora
- Acute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.DDocumento12 pagineAcute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.Dkerm6991Nessuna valutazione finora
- Ec Declaration of Conformity: W1/35 KEV KIRK - Protective Gloves - Cathegory IIDocumento3 pagineEc Declaration of Conformity: W1/35 KEV KIRK - Protective Gloves - Cathegory IICrystal HooverNessuna valutazione finora
- Dr. Sajjad Hussain Sumrra Isomerism (CHEM-305) Inorganic Chemistry-IIDocumento48 pagineDr. Sajjad Hussain Sumrra Isomerism (CHEM-305) Inorganic Chemistry-IITanya DilshadNessuna valutazione finora
- The Case - Lijjat PapadDocumento16 pagineThe Case - Lijjat Papadganesh572Nessuna valutazione finora
- Project Management A Technicians Guide Staples TOCDocumento5 pagineProject Management A Technicians Guide Staples TOCAnonymous NwnJNO0% (3)
- Brief RESUME EmailDocumento4 pagineBrief RESUME Emailranjit_kadalg2011Nessuna valutazione finora
- Bio411 C1Documento1 paginaBio411 C1Aqiena BalqisNessuna valutazione finora
- Medical Records in Family PracticeDocumento22 pagineMedical Records in Family PracticenurfadillahNessuna valutazione finora
- Viscoline Annular UnitDocumento4 pagineViscoline Annular UnitjoquispeNessuna valutazione finora
- Uas MR1Documento2 pagineUas MR1IvanNessuna valutazione finora
- Leather & Polymer - Lec01.2k11Documento11 pagineLeather & Polymer - Lec01.2k11Anik AlamNessuna valutazione finora
- Behavior Specific Praise Statements HandoutDocumento3 pagineBehavior Specific Praise Statements HandoutDaniel BernalNessuna valutazione finora
- Congenital Flexural Deformity in CalfDocumento6 pagineCongenital Flexural Deformity in CalfBibek SutradharNessuna valutazione finora
- Women EmpowermentDocumento7 pagineWomen EmpowermentJessica Glenn100% (1)
- 10 2005 Dec QDocumento6 pagine10 2005 Dec Qspinster40% (1)
- 2 Dawn150Documento109 pagine2 Dawn150kirubelNessuna valutazione finora
- D6228 - 10Documento8 pagineD6228 - 10POSSDNessuna valutazione finora
- Science 9 Q4 SML17 V2Documento15 pagineScience 9 Q4 SML17 V2HotdogNessuna valutazione finora
- Registration Statement (For Single Proprietor)Documento2 pagineRegistration Statement (For Single Proprietor)Sherwin SalanayNessuna valutazione finora
- Rules For State Competitions and Iabf Approved TournamentsDocumento56 pagineRules For State Competitions and Iabf Approved TournamentsQuality management systems documentsNessuna valutazione finora
- Birding The Gulf Stream: Inside This IssueDocumento5 pagineBirding The Gulf Stream: Inside This IssueChoctawhatchee Audubon SocietyNessuna valutazione finora
- Home Composting SystemsDocumento8 pagineHome Composting Systemssumanenthiran123Nessuna valutazione finora
- BV Lesson Plan 4Documento3 pagineBV Lesson Plan 4api-252119803Nessuna valutazione finora
- PMI Framework Processes PresentationDocumento17 paginePMI Framework Processes PresentationAakash BhatiaNessuna valutazione finora
- Present Continuous Exercises Test 1 - Positive Statements ExerciseDocumento2 paginePresent Continuous Exercises Test 1 - Positive Statements Exerciseangel omar peraltaNessuna valutazione finora
- United States v. Victor Vallin-Jauregui, 4th Cir. (2013)Documento4 pagineUnited States v. Victor Vallin-Jauregui, 4th Cir. (2013)Scribd Government DocsNessuna valutazione finora
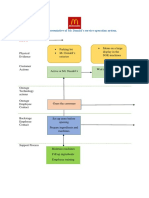
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocumento2 pagineBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNessuna valutazione finora