Potrebbero piacerti anche
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsDa EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNessuna valutazione finora
- Young Singles and Couples Product Summary: You Get With HCFDocumento4 pagineYoung Singles and Couples Product Summary: You Get With HCFJames SandersNessuna valutazione finora
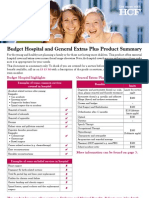
- Budget Hospital and General Extras Plus Product SummaryDocumento4 pagineBudget Hospital and General Extras Plus Product SummaryJames SandersNessuna valutazione finora
- HCF - Top PlusDocumento14 pagineHCF - Top PluscraivaimNessuna valutazione finora
- Corporate Classic PDFDocumento4 pagineCorporate Classic PDFironhide404Nessuna valutazione finora
- Advantage Blue: Summary of BenefitsDocumento4 pagineAdvantage Blue: Summary of BenefitsDeeDee JonesNessuna valutazione finora
- Kaiser Permanente: Good Health Is No SecretDocumento6 pagineKaiser Permanente: Good Health Is No SecretThomas Dominic CazneauNessuna valutazione finora
- Budget Hospital and Super Extras Cover: Question? Need Advice? Consultants Available To HelpDocumento11 pagineBudget Hospital and Super Extras Cover: Question? Need Advice? Consultants Available To HelpMaik SpaikNessuna valutazione finora
- Hospital Adv Sav General Extras PlusDocumento5 pagineHospital Adv Sav General Extras PlusferdiddleNessuna valutazione finora
- Bupa ClassicExtras NSW ACT 0415Documento3 pagineBupa ClassicExtras NSW ACT 0415Investor ProtegeNessuna valutazione finora
- Gold Extras Cover at a GlanceDocumento3 pagineGold Extras Cover at a GlanceLaura Leander WildeNessuna valutazione finora
- Blue Shield - Platinum Full Ppo 150 12 15Documento5 pagineBlue Shield - Platinum Full Ppo 150 12 15api-252555369Nessuna valutazione finora
- Blue-Cross-Premier-Platinum-Extra-Dental-Vision CareerDocumento8 pagineBlue-Cross-Premier-Platinum-Extra-Dental-Vision Careerapi-248930594Nessuna valutazione finora
- 2012 Blue Advantage Benefit TableDocumento3 pagine2012 Blue Advantage Benefit Tableapi-41207808Nessuna valutazione finora
- Benefit Summary: Your BenefitsDocumento14 pagineBenefit Summary: Your BenefitsmadhusoftechNessuna valutazione finora
- Additional Pages of ReportDocumento9 pagineAdditional Pages of ReportHiren PatelNessuna valutazione finora
- HMO Coverage DetailsDocumento5 pagineHMO Coverage DetailsKriszel Torreliza100% (1)
- 2011-12 Benefits BrochureDocumento4 pagine2011-12 Benefits BrochureKevin MarshallNessuna valutazione finora
- 2010 2011KaiserBenefitSummaryDocumento1 pagina2010 2011KaiserBenefitSummaryJim LombardoNessuna valutazione finora
- Blue Cross Select BronzeDocumento6 pagineBlue Cross Select Bronzeapi-285960909Nessuna valutazione finora
- Ins Flex Guideon 17Documento1 paginaIns Flex Guideon 17api-97071804Nessuna valutazione finora
- Kaiser Permanente: KP CA Silver 2000/45: This Is Only A SummaryDocumento8 pagineKaiser Permanente: KP CA Silver 2000/45: This Is Only A SummaryKelly HoffmanNessuna valutazione finora
- KP Dcgold020dentalpeddental IvlDocumento8 pagineKP Dcgold020dentalpeddental IvlKhamed TabetNessuna valutazione finora
- Bup I17 Wbms20rDocumento1 paginaBup I17 Wbms20rhn317Nessuna valutazione finora
- Bupa Young Singles ChoiceDocumento2 pagineBupa Young Singles Choicemisc1976Nessuna valutazione finora
- University of Missouri Kansas City International SBC 500499912071900371 FINAL 2Documento7 pagineUniversity of Missouri Kansas City International SBC 500499912071900371 FINAL 2maheshm_erpNessuna valutazione finora
- JACAM Benefit OverviewDocumento7 pagineJACAM Benefit OverviewStephenDohertyNessuna valutazione finora
- ITPPL HMO - IntellicareDocumento7 pagineITPPL HMO - IntellicarejsevillaonlineNessuna valutazione finora
- A Life Med Regular Brochure Full 201401Documento20 pagineA Life Med Regular Brochure Full 201401Loges Waran MohanNessuna valutazione finora
- Bins Lifeline Gold Ipid en Apr21 0024066Documento2 pagineBins Lifeline Gold Ipid en Apr21 0024066Shivay KundraNessuna valutazione finora
- Union Proposes Medicard as HMO for EmployeesDocumento31 pagineUnion Proposes Medicard as HMO for EmployeesDiorVelasquez100% (1)
- Medicaid Chip DetailsDocumento4 pagineMedicaid Chip DetailsJonathan CorbettNessuna valutazione finora
- HmoDocumento35 pagineHmoDiorVelasquezNessuna valutazione finora
- Health Insurance - Policy Year 2016: Frequently Asked QuestionsDocumento4 pagineHealth Insurance - Policy Year 2016: Frequently Asked QuestionsMuhammad Sarmad Ahsan0% (1)
- Plans Comparison SheetDocumento1 paginaPlans Comparison SheetDayanand WasateNessuna valutazione finora
- Compare Private Health Insurance PoliciesDocumento16 pagineCompare Private Health Insurance PoliciesNamhar AnimasNessuna valutazione finora
- Medical Coverage For Non-U.s. Citizens Visiting The U.SDocumento9 pagineMedical Coverage For Non-U.s. Citizens Visiting The U.SsandakaaaNessuna valutazione finora
- Schedule of BenefitsDocumento7 pagineSchedule of BenefitsMaddy CruzNessuna valutazione finora
- Daman Select Gold InclusionsDocumento2 pagineDaman Select Gold InclusionsmukeshsinghtomarNessuna valutazione finora
- Your Medicare Benefits 2014Documento63 pagineYour Medicare Benefits 2014mpersiNessuna valutazione finora
- DWN HV Brochure 0829Documento7 pagineDWN HV Brochure 0829Marquis C Jones Sr.Nessuna valutazione finora
- Insurance Benefit SummaryDocumento4 pagineInsurance Benefit SummaryRose Mary Read BallNessuna valutazione finora
- CIEE Insurance CoverageDocumento2 pagineCIEE Insurance CoverageMiguelNessuna valutazione finora
- Employee Benefits-Wellness Guide 2023-24Documento30 pagineEmployee Benefits-Wellness Guide 2023-24shanzeh2609Nessuna valutazione finora
- I A Bluechoice Ppo - Large Group (51+ Employees) Plan 4511Sx Benefit SummaryDocumento3 pagineI A Bluechoice Ppo - Large Group (51+ Employees) Plan 4511Sx Benefit SummaryDave EmersonNessuna valutazione finora
- Anthem Classic PPO 250-20-20Documento4 pagineAnthem Classic PPO 250-20-20PhilippNessuna valutazione finora
- ACDocumento4 pagineACNrc A.Nessuna valutazione finora
- Protect What You Treasure Most: HealthDocumento12 pagineProtect What You Treasure Most: HealthNelly HNessuna valutazione finora
- Our Dental Plan For Individuals and FamiliesDocumento4 pagineOur Dental Plan For Individuals and Familiesapi-41207808Nessuna valutazione finora
- Outpatient One Pager Version 1.0 Apr 20Documento1 paginaOutpatient One Pager Version 1.0 Apr 20naval730107Nessuna valutazione finora
- AARP UHC 2024 Benefit Highlights LA 004P FocusDocumento4 pagineAARP UHC 2024 Benefit Highlights LA 004P FocusAlaa ZaidNessuna valutazione finora
- 2012 Hsa Benefit TableDocumento3 pagine2012 Hsa Benefit Tableapi-41207808Nessuna valutazione finora
- Star Out Patient Care Insurance PolicyV 1.0may2023Documento37 pagineStar Out Patient Care Insurance PolicyV 1.0may2023ठाकुर सूरज राणाNessuna valutazione finora
- Your guide to 70% back on included extras with black 70 boostDocumento6 pagineYour guide to 70% back on included extras with black 70 boostSaifuddin SidikiNessuna valutazione finora
- IPID - Silver CLICE Expat - EN - 05 - 2022Documento2 pagineIPID - Silver CLICE Expat - EN - 05 - 2022invoices invoicesNessuna valutazione finora
- Medicare AetnaplanbenefitsDocumento22 pagineMedicare AetnaplanbenefitsBert GeorgeNessuna valutazione finora
- Essential Lite Brochure Benefits and CoverageDocumento10 pagineEssential Lite Brochure Benefits and CoveragePoekie123456Nessuna valutazione finora
- HealthDocumento1 paginaHealthrcdasariNessuna valutazione finora
- Sample PDFDocumento10 pagineSample PDFkumarank12Nessuna valutazione finora
- ACT Compass TestDocumento11 pagineACT Compass TestJorge PageNessuna valutazione finora
- ACT Compass TestDocumento11 pagineACT Compass TestJorge PageNessuna valutazione finora
- Sample PDFDocumento10 pagineSample PDFkumarank12Nessuna valutazione finora
- Ofm MSFT Interop v5c 132827Documento53 pagineOfm MSFT Interop v5c 132827rcdasariNessuna valutazione finora
- ACT Compass TestDocumento11 pagineACT Compass TestJorge PageNessuna valutazione finora
- SamlDocumento8 pagineSamlrcdasariNessuna valutazione finora
- R12 Istore SSO WhitepaperDocumento46 pagineR12 Istore SSO WhitepaperrcdasariNessuna valutazione finora
- Oracle Istore Implementation AdminDocumento1.062 pagineOracle Istore Implementation AdminkmehsramNessuna valutazione finora
- Oracle Istore Implementation AdminDocumento1.062 pagineOracle Istore Implementation AdminkmehsramNessuna valutazione finora
- Living With CancerDocumento400 pagineLiving With CancerAnonymous FGqnrDuMNessuna valutazione finora
- Repositioning an Inverted UterusDocumento5 pagineRepositioning an Inverted Uterusshraddha vermaNessuna valutazione finora
- SimChart Charting RequirementsDocumento3 pagineSimChart Charting RequirementsMatt McClenahanNessuna valutazione finora
- Electrical Burn PathophysiologyDocumento1 paginaElectrical Burn PathophysiologydanicaNessuna valutazione finora
- Nursing Management of Nephrotic SyndromeDocumento2 pagineNursing Management of Nephrotic SyndromeMARYAM AL-KADHIMNessuna valutazione finora
- Cannabis-An IntroductionDocumento5 pagineCannabis-An IntroductionSaleha TariqNessuna valutazione finora
- Intermittent Fasting A GuideDocumento20 pagineIntermittent Fasting A Guidedddaaaappp83% (6)
- Adrenaline - EpinephrineDocumento3 pagineAdrenaline - Epinephrinesweety DangiNessuna valutazione finora
- Organization of NICU ServicesDocumento45 pagineOrganization of NICU ServicesMonika Bagchi84% (64)
- Organ Systems InterviewDocumento2 pagineOrgan Systems InterviewJohn Carlo MontemayorNessuna valutazione finora
- UabDocumento20 pagineUabAnonymous n7RT07fzUdNessuna valutazione finora
- Breast and Nipple Thrush - 280720Documento6 pagineBreast and Nipple Thrush - 280720Robbie WilliamsNessuna valutazione finora
- Buteyko Meets DR MewDocumento176 pagineButeyko Meets DR MewAnonymous hndaj8zCA100% (1)
- Agni Dagdha. Group-T Patients Were Treated With Indigenous Drugs and Group-C PatientsDocumento14 pagineAgni Dagdha. Group-T Patients Were Treated With Indigenous Drugs and Group-C PatientsKrishnaNessuna valutazione finora
- Patient'S Peripheral Arterial Disease Risk FactorsDocumento2 paginePatient'S Peripheral Arterial Disease Risk FactorsKrystel BatinoNessuna valutazione finora
- Course and Practicum ReflectionsDocumento34 pagineCourse and Practicum Reflectionsapi-554096544Nessuna valutazione finora
- Gender-Dysphoric-Incongruene Persons, Guidelines JCEM 2017Documento35 pagineGender-Dysphoric-Incongruene Persons, Guidelines JCEM 2017Manel EMNessuna valutazione finora
- TOPIC 3.A Bag TechniqueDocumento38 pagineTOPIC 3.A Bag TechniqueJayrelle D. Safran100% (1)
- Aiims Hospital Disaster PlanDocumento6 pagineAiims Hospital Disaster PlanSujatha J JayabalNessuna valutazione finora
- ImgDocumento1 paginaImgLIDIYA MOL P V100% (1)
- Approved Private Hospitals List for CG Govt EmployeesDocumento12 pagineApproved Private Hospitals List for CG Govt Employeesm_asitNessuna valutazione finora
- Role of IV Meropenem in Current EraDocumento38 pagineRole of IV Meropenem in Current EraImtiyaz Alam SahilNessuna valutazione finora
- Practices of Self-Medication Among Tribal Population North Maharashtra (Khandesh)Documento5 paginePractices of Self-Medication Among Tribal Population North Maharashtra (Khandesh)Latasha WilderNessuna valutazione finora
- NCA - CVA InfarctDocumento126 pagineNCA - CVA InfarctRosaree Mae PantojaNessuna valutazione finora
- Hospital Information Management System - Cover PageDocumento15 pagineHospital Information Management System - Cover Pageapi-1946401583% (6)
- Approach To Neurologic Infections.4 PDFDocumento18 pagineApproach To Neurologic Infections.4 PDFosmarfalboreshotmail.comNessuna valutazione finora
- Fistulas Enterocutaneas MaingotDocumento20 pagineFistulas Enterocutaneas MaingotroyvillafrancaNessuna valutazione finora
- AssociationBetweenBRAFV600EMutationand MortalityDocumento9 pagineAssociationBetweenBRAFV600EMutationand MortalityMade RusmanaNessuna valutazione finora
- Trigeminal Neuralgia GuideDocumento15 pagineTrigeminal Neuralgia Guideandreas kevinNessuna valutazione finora