Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
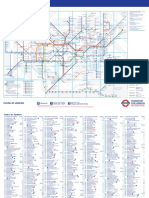
- Standard Tube MapDocumento2 pagineStandard Tube MapBenjamin Zari IIINessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Hines Chaps 1 5 6 10 11Documento19 pagineHines Chaps 1 5 6 10 11dominscience1Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Canterbury PDFDocumento1 paginaCanterbury PDFdominscience1Nessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Cognitive PsychologyDocumento10 pagineCognitive Psychologydominscience1Nessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hansen, G - Deception in PSI ResearchDocumento57 pagineHansen, G - Deception in PSI Researchdominscience1Nessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Moller, L - Pseudoscience or ProtoscienceDocumento3 pagineMoller, L - Pseudoscience or Protosciencedominscience1Nessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Moller, L - Pseudoscience or ProtoscienceDocumento3 pagineMoller, L - Pseudoscience or Protosciencedominscience1Nessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hansen, G - Deception in PSI ResearchDocumento57 pagineHansen, G - Deception in PSI Researchdominscience1Nessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- DialoguesClinNeurosci 9 173Documento17 pagineDialoguesClinNeurosci 9 173dominscience1Nessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Cognitive PsychologyDocumento10 pagineCognitive Psychologydominscience1Nessuna valutazione finora
- Reader, C - Khufu Knew The SphinxDocumento19 pagineReader, C - Khufu Knew The Sphinxdominscience1Nessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Cognitive PsychologyDocumento10 pagineCognitive Psychologydominscience1Nessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Spirit Slate Writing and Kindred PhenomenaDocumento89 pagineSpirit Slate Writing and Kindred Phenomenadominscience1Nessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Playing Ground PartIDocumento3 pagineThe Playing Ground PartIdominscience1Nessuna valutazione finora
- Did A Five-Day Camp Without Digital Devices Really Boost Children's Interpersonal Skills?Documento2 pagineDid A Five-Day Camp Without Digital Devices Really Boost Children's Interpersonal Skills?dominscience1Nessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Breaking ResearchDocumento2 pagineBreaking Researchdominscience1Nessuna valutazione finora
- Using "Programmable" Antibiotics To Attack Drug-Resistant MicrobesDocumento3 pagineUsing "Programmable" Antibiotics To Attack Drug-Resistant Microbesdominscience1Nessuna valutazione finora
- The Playing Ground PartDocumento3 pagineThe Playing Ground Partdominscience1Nessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Tricksy Insects Sing A Song of Love andDocumento2 pagineTricksy Insects Sing A Song of Love anddominscience1Nessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Neurobiological Basis of A HumanDocumento3 pagineThe Neurobiological Basis of A Humandominscience1Nessuna valutazione finora
- Sleeping Brains Understand WordsDocumento2 pagineSleeping Brains Understand Wordsdominscience1Nessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The GutDocumento2 pagineThe Gutdominscience1Nessuna valutazione finora
- Epidural AnalgesiaDocumento16 pagineEpidural AnalgesiaspreeasNessuna valutazione finora
- MCQ AnaesthesiaDocumento15 pagineMCQ AnaesthesiaProf-Ashraf Emara100% (2)
- Evaluation and Management of Pain in ChildrenDocumento13 pagineEvaluation and Management of Pain in ChildrenOlga MoţpanNessuna valutazione finora
- Jex Review Center Marathon in Criminal Detection and InvestigationDocumento4 pagineJex Review Center Marathon in Criminal Detection and InvestigationArnel Sali-otNessuna valutazione finora
- PharmacologyAnesthesiology RevalidaDocumento166 paginePharmacologyAnesthesiology RevalidaKENT DANIEL SEGUBIENSE100% (1)
- Anes 8 Introduction To Pain ManagementDocumento4 pagineAnes 8 Introduction To Pain ManagementJanica Marie RagsacNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- GP MCQ 11Documento4 pagineGP MCQ 11Marta MoreiraNessuna valutazione finora
- Xylazine-Involved Overdose Deaths FINAL - 3.8.23Documento5 pagineXylazine-Involved Overdose Deaths FINAL - 3.8.23ActionNewsJaxNessuna valutazione finora
- TCCC Guidelines For Medical Personnel 150603Documento14 pagineTCCC Guidelines For Medical Personnel 150603Vitor Hugo G CorreiaNessuna valutazione finora
- Acute Post-Surgical Pain Management: A Critical Appraisal of Current PracticeDocumento42 pagineAcute Post-Surgical Pain Management: A Critical Appraisal of Current PracticeMmenyeneNessuna valutazione finora
- Drug Study ShenDocumento12 pagineDrug Study ShenLass KazeNessuna valutazione finora
- Case AppendicitisDocumento112 pagineCase AppendicitisChen CobainNessuna valutazione finora
- Summativeassessment 3Documento11 pagineSummativeassessment 3api-522946517Nessuna valutazione finora
- 1756 9966 29 67Documento6 pagine1756 9966 29 67Yogha RyanandaNessuna valutazione finora
- 1 s2.0 S0898656821000693 MainDocumento4 pagine1 s2.0 S0898656821000693 MainLívia MeloNessuna valutazione finora
- Generic Name: Frequent (10%) Baseline Assessment Antiemetic (Assess Intervention/EvaluationDocumento11 pagineGeneric Name: Frequent (10%) Baseline Assessment Antiemetic (Assess Intervention/EvaluationIrene Soriano BayubayNessuna valutazione finora
- Rusan Pharma Product ListDocumento4 pagineRusan Pharma Product ListSanjay SharmaNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- DS - DutyDocumento19 pagineDS - DutyMarie Kelsey Acena MacaraigNessuna valutazione finora
- Drug TraffickingDocumento20 pagineDrug TraffickingUsman Ahmad TijjaniNessuna valutazione finora
- Concise Guide To Medicine & Drugs, 7th Edition by DKDocumento498 pagineConcise Guide To Medicine & Drugs, 7th Edition by DKJosh MNessuna valutazione finora
- S 006 LBLDocumento21 pagineS 006 LBLEko YuliantoNessuna valutazione finora
- ZOMORPH Capsules 10mgDocumento6 pagineZOMORPH Capsules 10mgFlorexan Malanday PasonNessuna valutazione finora
- Artigo Produtos NaturaisDocumento39 pagineArtigo Produtos NaturaisMillygoNessuna valutazione finora
- Hridae Walia Interaction Design Portfolio PDFDocumento114 pagineHridae Walia Interaction Design Portfolio PDFHridae WaliaNessuna valutazione finora
- Pollice Et Al 2008 Severe Tramadol Addiction in A 61 Year Old Woman Without A History of Substance AbuseDocumento2 paginePollice Et Al 2008 Severe Tramadol Addiction in A 61 Year Old Woman Without A History of Substance Abusefernyz2886Nessuna valutazione finora
- Pain Management JournalDocumento7 paginePain Management JournalPengurus Pusat HipgabiNessuna valutazione finora
- Concept Of: (The Fifth Vital Sign)Documento43 pagineConcept Of: (The Fifth Vital Sign)Mae DacerNessuna valutazione finora
- What Are Drug ClassificationsDocumento5 pagineWhat Are Drug ClassificationsCarl LewisNessuna valutazione finora
- MRQ Base For Final Exam PreparationsDocumento29 pagineMRQ Base For Final Exam PreparationssushmitaNessuna valutazione finora
- Pharmacology NotesDocumento30 paginePharmacology NotesJessica WalkerNessuna valutazione finora
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora