Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Reincarnated As A Sword Volume 12Documento263 pagineReincarnated As A Sword Volume 12Phil100% (1)
- Niche Market Tourism (Autosaved) PowerPointDocumento83 pagineNiche Market Tourism (Autosaved) PowerPointkamilahNessuna valutazione finora
- TC1 Response To A Live Employer Brief: Module Code: BSOM084Documento16 pagineTC1 Response To A Live Employer Brief: Module Code: BSOM084syeda maryemNessuna valutazione finora
- Debt Policy and Firm Performance of Family Firms The Impact of Economic AdversityDocumento21 pagineDebt Policy and Firm Performance of Family Firms The Impact of Economic AdversityMiguel Hernandes JuniorNessuna valutazione finora
- EF 3rd Upper Interm File 8 TEST PDFDocumento4 pagineEF 3rd Upper Interm File 8 TEST PDFfriboNessuna valutazione finora
- Performance AnalyticsDocumento193 paginePerformance AnalyticsGNessuna valutazione finora
- Fine Art Dissertation ConclusionDocumento4 pagineFine Art Dissertation ConclusionBuyALiteratureReviewPaperUK100% (1)
- 0 - Past Simple TenseDocumento84 pagine0 - Past Simple Tenseשחר וולפסוןNessuna valutazione finora
- Tool - Single Double Triple Loop LearningDocumento2 pagineTool - Single Double Triple Loop LearningDwiAryantiNessuna valutazione finora
- Shaft KeywayDocumento8 pagineShaft KeywayturboconchNessuna valutazione finora
- Jurisprudence Notes - Customs, Precedents & LegislationsDocumento30 pagineJurisprudence Notes - Customs, Precedents & LegislationsBhumijaNessuna valutazione finora
- 50 Interview Questions For Adryenn AshleyDocumento5 pagine50 Interview Questions For Adryenn AshleyAdryenn AshleyNessuna valutazione finora
- Definition of Diplomatic AgentDocumento3 pagineDefinition of Diplomatic AgentAdv Faisal AwaisNessuna valutazione finora
- Product Manual 85018V2 (Revision F) : 505E Digital Governor For Extraction Steam TurbinesDocumento160 pagineProduct Manual 85018V2 (Revision F) : 505E Digital Governor For Extraction Steam Turbinesrahilshah100Nessuna valutazione finora
- How Is The Frog's Stomach Adapted To Provide An Increased Digestive Surface?Documento6 pagineHow Is The Frog's Stomach Adapted To Provide An Increased Digestive Surface?Jemuel Bucud LagartoNessuna valutazione finora
- LESSON 1 Overview of Toeic Speaking WritingDocumento29 pagineLESSON 1 Overview of Toeic Speaking WritingPhạm Thị HuyềnNessuna valutazione finora
- A Seminar Report On Soft Skills: Submitted To Visvesvaraya Technological University, BelgaumDocumento18 pagineA Seminar Report On Soft Skills: Submitted To Visvesvaraya Technological University, Belgaumvishal vallapure100% (1)
- Daad-Courses-2019-09-08 6Documento91 pagineDaad-Courses-2019-09-08 6Kaushik RajNessuna valutazione finora
- Speculative DesignDocumento16 pagineSpeculative DesignWill Kurlinkus100% (1)
- Expansion and Contraction of Demand:: Change in Demand vs. Change in Quantity DemandedDocumento6 pagineExpansion and Contraction of Demand:: Change in Demand vs. Change in Quantity DemandedbadarNessuna valutazione finora
- Jacob Marries Leah and RachelDocumento1 paginaJacob Marries Leah and RacheljellyB RafaelNessuna valutazione finora
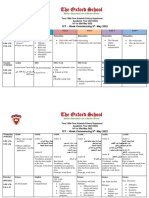
- Term 3 Mid-Term Assessment ScheduleDocumento9 pagineTerm 3 Mid-Term Assessment ScheduleRabia MoeedNessuna valutazione finora
- Best Resume Template CanadaDocumento4 pagineBest Resume Template Canadaafjwdprlzaxewj100% (2)
- Karling Aguilera-Fort ResumeDocumento4 pagineKarling Aguilera-Fort Resumeapi-3198760590% (1)
- Chap 005Documento13 pagineChap 005Mohammad ElabedNessuna valutazione finora
- Case Theory BigamyDocumento6 pagineCase Theory BigamyLouem GarceniegoNessuna valutazione finora
- Marketing Ethics Amal 12-09-10Documento11 pagineMarketing Ethics Amal 12-09-10amalroy1986Nessuna valutazione finora
- Knowledge Versus OpinionDocumento20 pagineKnowledge Versus OpinionShumaila HameedNessuna valutazione finora
- Test 04 AnswerDocumento16 pagineTest 04 AnswerCửu KhoaNessuna valutazione finora
- Sample Legal Advice Problems and AnswersDocumento4 pagineSample Legal Advice Problems and AnswersJake Bryson DancelNessuna valutazione finora