Potrebbero piacerti anche
- (Therapy in Practice Series) Rosemary Gravell, Jenny France (Auth.) - Speech and Communication Problems in Psychiatry (1991, Springer US) PDFDocumento364 pagine(Therapy in Practice Series) Rosemary Gravell, Jenny France (Auth.) - Speech and Communication Problems in Psychiatry (1991, Springer US) PDFmelike50% (2)
- Hashimoto Thyroiditis, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandHashimoto Thyroiditis, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Chronic IllnessDocumento12 pagineChronic IllnessRegineCuasSulib100% (2)
- Sample Interview Questions For TeachersDocumento11 pagineSample Interview Questions For TeachersRegineCuasSulibNessuna valutazione finora
- A Case Presentation On Multinodular GoitreDocumento27 pagineA Case Presentation On Multinodular Goitrecnsatish86% (7)
- Pathophysiology of HyperthyroidismDocumento97 paginePathophysiology of HyperthyroidismMarie Joyce SablanNessuna valutazione finora
- Medical Kit Components EandEDocumento54 pagineMedical Kit Components EandETroy Ashcraft100% (2)
- Pathophysiology of COPDDocumento42 paginePathophysiology of COPDRegineCuasSulib100% (3)
- Stop The Thyroid Madness Sanjay Dixit MDDocumento68 pagineStop The Thyroid Madness Sanjay Dixit MDdb50% (2)
- Magnets and Pain Relief Project CompleteDocumento6 pagineMagnets and Pain Relief Project Completeapi-356214846100% (3)
- Pathophysiology of EndocrinologyDocumento25 paginePathophysiology of EndocrinologyISRAELNessuna valutazione finora
- Hashimoto ThyroiditisDocumento6 pagineHashimoto Thyroiditismananginsiang100% (1)
- Caregiving Final 2nd Sem ExamDocumento3 pagineCaregiving Final 2nd Sem ExamRichard CortezNessuna valutazione finora
- Ambulating ClientDocumento4 pagineAmbulating ClientRegineCuasSulibNessuna valutazione finora
- 8 - Sullivan - Interpersonal TheoryDocumento4 pagine8 - Sullivan - Interpersonal TheorystephanieNessuna valutazione finora
- Tesis vITAMIN C CONTENT IN FRUITSDocumento24 pagineTesis vITAMIN C CONTENT IN FRUITSHema JothyNessuna valutazione finora
- LipidsDocumento25 pagineLipidsJeaniee Zosa Ebias50% (10)
- Family Genogram ArticleDocumento26 pagineFamily Genogram Articleaawulff100% (3)
- Diseases of The Thyroid Gland PDFDocumento72 pagineDiseases of The Thyroid Gland PDFKay BristolNessuna valutazione finora
- Staphylococcus Aureus and Other Staphylococci Are TheDocumento3 pagineStaphylococcus Aureus and Other Staphylococci Are TheRaphael Reyes EnriquezNessuna valutazione finora
- When Did Mr. Jones First Have Symptoms or Problems? How Long Has This Been Happening?Documento3 pagineWhen Did Mr. Jones First Have Symptoms or Problems? How Long Has This Been Happening?RegineCuasSulibNessuna valutazione finora
- Thyroid StormDocumento11 pagineThyroid StormAndrew UtamaNessuna valutazione finora
- Thyroid It IsDocumento16 pagineThyroid It IsRoby KieranNessuna valutazione finora
- Thyroiditis: o o o o o oDocumento10 pagineThyroiditis: o o o o o omagisasamundoNessuna valutazione finora
- Hypothyroidis SecondaryDocumento4 pagineHypothyroidis SecondaryfynneroNessuna valutazione finora
- Hyperthyroidism and Thyrotoxicosis: Practice EssentialsDocumento39 pagineHyperthyroidism and Thyrotoxicosis: Practice Essentialssyl viNessuna valutazione finora
- Thyroiditis: Uaepong Limpapanasit 23/5/54Documento36 pagineThyroiditis: Uaepong Limpapanasit 23/5/54Rapid MedicineNessuna valutazione finora
- Tyroid StormDocumento10 pagineTyroid StormAfdhalia Khairunnisa SyammarhanNessuna valutazione finora
- Hyperthyroidism, Thyroid Storm, and Graves Disease: BackgroundDocumento22 pagineHyperthyroidism, Thyroid Storm, and Graves Disease: BackgroundAnonymous 3OoumAUytNessuna valutazione finora
- Endocrine System: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocumento32 pagineEndocrine System: Dr. I Made Naris Pujawan, M.Biomed, SP - PADewi SofyanaNessuna valutazione finora
- Thyroid Storm May Be The Initial Presentation Of: Thyrotoxicosis in Undiagnosed Children, Particularly in NeonatesDocumento8 pagineThyroid Storm May Be The Initial Presentation Of: Thyrotoxicosis in Undiagnosed Children, Particularly in NeonatesLolla MorsiNessuna valutazione finora
- Hyperthyroidism and Thyrotoxicosis - Practice Essentials, Background, PathophysiologyDocumento13 pagineHyperthyroidism and Thyrotoxicosis - Practice Essentials, Background, Pathophysiologyabenezer g/kirstosNessuna valutazione finora
- Hypothyroidism: Prepared By: Angel Shwaihat Enas Khamaiseh Supervised By: Dr. Khalil Al SoutariDocumento33 pagineHypothyroidism: Prepared By: Angel Shwaihat Enas Khamaiseh Supervised By: Dr. Khalil Al Soutariraed faisalNessuna valutazione finora
- Subacute, Silent, and Postpartum Thyroiditis 2012Documento11 pagineSubacute, Silent, and Postpartum Thyroiditis 2012YoaNnita GoMezNessuna valutazione finora
- Hypothyroidism: Special Types of HypothyroidismDocumento4 pagineHypothyroidism: Special Types of HypothyroidismVictor VicencioNessuna valutazione finora
- Chronic Thyroid It IsDocumento3 pagineChronic Thyroid It IsTonio PagaoNessuna valutazione finora
- Background: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureDocumento8 pagineBackground: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureIkmal HazliNessuna valutazione finora
- Morning ReportDocumento31 pagineMorning Reports1882Nessuna valutazione finora
- Bening Disease of Thyroid GlandDocumento85 pagineBening Disease of Thyroid GlandKarishma MishraNessuna valutazione finora
- Tiroiditis Subakut PDFDocumento8 pagineTiroiditis Subakut PDFAdeh MahardikaNessuna valutazione finora
- Hyperthyroidism and ThyrotoxicosisDocumento33 pagineHyperthyroidism and Thyrotoxicosiseze033Nessuna valutazione finora
- Hyperthyroidism in Children: Houssam Fayad, MDDocumento34 pagineHyperthyroidism in Children: Houssam Fayad, MDHoussam FayadNessuna valutazione finora
- Wo Week 4 (Hyperthyroidism)Documento12 pagineWo Week 4 (Hyperthyroidism)Theddyon BhenlieNessuna valutazione finora
- EndocrinologyDocumento39 pagineEndocrinologySoumyajit Ray ChaudhuriNessuna valutazione finora
- Hyperthyroidism and Thyrotoxicosis PDFDocumento16 pagineHyperthyroidism and Thyrotoxicosis PDFMuhammad IkbarNessuna valutazione finora
- Thyroid StormDocumento36 pagineThyroid StormSabrina ShalhoutNessuna valutazione finora
- Internal Med. EndoDocumento35 pagineInternal Med. EndoEdwin OkonNessuna valutazione finora
- 4.thyroiditis MedlineDocumento11 pagine4.thyroiditis MedlineDayatPettasiriNessuna valutazione finora
- Background: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureDocumento13 pagineBackground: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureFebria ArmaNessuna valutazione finora
- Hypothyroidism: ClassificationDocumento9 pagineHypothyroidism: Classificationpali_sakshamNessuna valutazione finora
- Bta Patient Hyperthyroidism PDFDocumento4 pagineBta Patient Hyperthyroidism PDFWILLIAMNessuna valutazione finora
- Hypothyroidism Evaluation of Thyroid FunctionDocumento9 pagineHypothyroidism Evaluation of Thyroid FunctionJJ hidden objectNessuna valutazione finora
- HyperthyroidismDocumento12 pagineHyperthyroidismShoppe 'n ShoppersNessuna valutazione finora
- Hyperthyroidism 1Documento88 pagineHyperthyroidism 1Mamikie Vukeya100% (1)
- Thyroiditis: What Is The Thyroid Gland?Documento3 pagineThyroiditis: What Is The Thyroid Gland?husni gunawanNessuna valutazione finora
- Tutorial 2 Modul 1 Blok 21Documento12 pagineTutorial 2 Modul 1 Blok 21chitra safaNessuna valutazione finora
- Benign Thyroid DiseasesDocumento8 pagineBenign Thyroid DiseasesBkas GrgNessuna valutazione finora
- Hyperthyroidism: Sudiarto, MNDocumento21 pagineHyperthyroidism: Sudiarto, MNerikaNessuna valutazione finora
- ThyrotoxicosisDocumento15 pagineThyrotoxicosischrysandre100% (1)
- Hashimoto Thyroiditis: Practice EssentialsDocumento5 pagineHashimoto Thyroiditis: Practice EssentialsĐặng Quỳnh ANNessuna valutazione finora
- Hyperthyoidism: Anaesthetic ManagementDocumento11 pagineHyperthyoidism: Anaesthetic ManagementerzaraptorNessuna valutazione finora
- Hperthyroidism 1Documento4 pagineHperthyroidism 1Salwa KaramanNessuna valutazione finora
- MerjohnDocumento4 pagineMerjohnMerjohn LibutonNessuna valutazione finora
- Thyroid Benign TumorDocumento30 pagineThyroid Benign TumormackieccNessuna valutazione finora
- Benign Thyroid Diseases NabeehDocumento69 pagineBenign Thyroid Diseases NabeehAli YousefNessuna valutazione finora
- Thyroiditis: Archana Bindra, M.D., and Glenn D. Braunstein, M.DDocumento8 pagineThyroiditis: Archana Bindra, M.D., and Glenn D. Braunstein, M.DanggrainiNessuna valutazione finora
- Overview of Thyroiditis - UpToDateDocumento7 pagineOverview of Thyroiditis - UpToDateCamila NogueiraNessuna valutazione finora
- Kuliah HyperthyroidDocumento18 pagineKuliah HyperthyroidFreddyNessuna valutazione finora
- Thyroid+Storm+ +StatPearls+ +NCBI+Bookshelf 1666577389538Documento9 pagineThyroid+Storm+ +StatPearls+ +NCBI+Bookshelf 1666577389538Novita Sri MulyatiNessuna valutazione finora
- Thyroiditis: What Is The Thyroid Gland?Documento3 pagineThyroiditis: What Is The Thyroid Gland?Angga M RahmanNessuna valutazione finora
- Thyroid: TRH TSHDocumento6 pagineThyroid: TRH TSHAjay Pal NattNessuna valutazione finora
- Thyroid Benign 2003 0514Documento30 pagineThyroid Benign 2003 0514cafemedNessuna valutazione finora
- Euthyroid Sick Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandEuthyroid Sick Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Health EducationDocumento8 pagineHealth EducationRegineCuasSulibNessuna valutazione finora
- Purchase Slip NoDocumento2 paginePurchase Slip NoRegineCuasSulibNessuna valutazione finora
- PnuemoniaDocumento102 paginePnuemoniaRegineCuasSulibNessuna valutazione finora
- The Concept of Powerlessness in Patient Treatment Nursing EssayDocumento38 pagineThe Concept of Powerlessness in Patient Treatment Nursing EssayreginesulibNessuna valutazione finora
- Cardiovascular SystemDocumento4 pagineCardiovascular SystemRegineCuasSulibNessuna valutazione finora
- Types of IV FluidsDocumento1 paginaTypes of IV FluidsRegineCuasSulibNessuna valutazione finora
- What Is Epilepsy?Documento10 pagineWhat Is Epilepsy?RegineCuasSulibNessuna valutazione finora
- Tissue Layers and IncisionsDocumento19 pagineTissue Layers and IncisionsRegineCuasSulibNessuna valutazione finora
- Diverticulitis PathophysiologyDocumento1 paginaDiverticulitis PathophysiologyreginesulibNessuna valutazione finora
- AbstractDocumento1 paginaAbstractRegineCuasSulibNessuna valutazione finora
- Diverticulitis PathophysiologyDocumento1 paginaDiverticulitis PathophysiologyreginesulibNessuna valutazione finora
- Renal System DisorderDocumento34 pagineRenal System DisorderRegineCuasSulibNessuna valutazione finora
- Cancer, Dementia & StrokeDocumento80 pagineCancer, Dementia & StrokeRegineCuasSulibNessuna valutazione finora
- Vacuum DeliveryDocumento2 pagineVacuum DeliveryRegineCuasSulibNessuna valutazione finora
- Types of IV FluidsDocumento1 paginaTypes of IV FluidsRegineCuasSulibNessuna valutazione finora
- What Is Epilepsy?Documento10 pagineWhat Is Epilepsy?RegineCuasSulibNessuna valutazione finora
- Chemistry Laboratory Result 1Documento10 pagineChemistry Laboratory Result 1RegineCuasSulibNessuna valutazione finora
- Regine ShockDocumento6 pagineRegine ShockRegineCuasSulibNessuna valutazione finora
- Liver CirrhosisDocumento6 pagineLiver CirrhosisRegineCuasSulibNessuna valutazione finora
- Chapter 1 Developmental Disorders of The Oral CavityDocumento6 pagineChapter 1 Developmental Disorders of The Oral CavityArafat Masud NiloyNessuna valutazione finora
- NRSG - Documentation and Quality Management in IvtDocumento12 pagineNRSG - Documentation and Quality Management in IvtRamon Carlo AlmiranezNessuna valutazione finora
- Surg LogBook Summary June 2019Documento15 pagineSurg LogBook Summary June 2019tameem100% (1)
- ResumeDocumento4 pagineResumeapi-283952616Nessuna valutazione finora
- Presentation 2017 ENGDocumento20 paginePresentation 2017 ENGpabloNessuna valutazione finora
- Basic TB FactsDocumento8 pagineBasic TB FactshatemfaroukNessuna valutazione finora
- Ati Communication NR 341 PDFDocumento3 pagineAti Communication NR 341 PDFmp1757Nessuna valutazione finora
- 01 - Onsite Sanitation TechnologiesDocumento80 pagine01 - Onsite Sanitation TechnologiesDivyam ShreevatsalNessuna valutazione finora
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocumento3 pagineAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNessuna valutazione finora
- High Purity Excipients GuideDocumento8 pagineHigh Purity Excipients GuideSA100% (1)
- Anaemia: by Swaathi R Final Year MbbsDocumento33 pagineAnaemia: by Swaathi R Final Year MbbsGopi NathNessuna valutazione finora
- Jaw Opening Exercises Head and Neck Cancer - Jun21Documento2 pagineJaw Opening Exercises Head and Neck Cancer - Jun21FalconNessuna valutazione finora
- Plaque ControlDocumento52 paginePlaque ControlIbrahim AbdelHadi100% (1)
- Final Composting ProposalDocumento26 pagineFinal Composting ProposalgreatgeniusNessuna valutazione finora
- Obstetric Nursing Care PlanDocumento12 pagineObstetric Nursing Care PlanfiercesheNessuna valutazione finora
- CAM101 Complete Course Notes Reduced SizeDocumento174 pagineCAM101 Complete Course Notes Reduced SizehaydenfarquharNessuna valutazione finora
- Hypokalemic Periodic ParalysisDocumento2 pagineHypokalemic Periodic ParalysissakuraleeshaoranNessuna valutazione finora
- IRBD Scales Abnormal Involuntary Movement ScaleDocumento2 pagineIRBD Scales Abnormal Involuntary Movement ScaleRoberto LlanesNessuna valutazione finora
- Neuropsychologia: Jade Dignam, David Copland, Alicia Rawlings, Kate O 'Brien, Penni Burfein, Amy D. RodriguezDocumento12 pagineNeuropsychologia: Jade Dignam, David Copland, Alicia Rawlings, Kate O 'Brien, Penni Burfein, Amy D. RodriguezFrancisco Beltrán NavarroNessuna valutazione finora
- ACM812 Ventilator - ASCFDocumento1 paginaACM812 Ventilator - ASCFMoussa ToudjaniNessuna valutazione finora
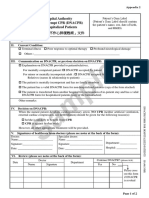
- Sample: Hospital Authority Do Not Attempt CPR (DNACPR) For Hospitalized PatientsDocumento2 pagineSample: Hospital Authority Do Not Attempt CPR (DNACPR) For Hospitalized PatientsSabilatul AbidahNessuna valutazione finora
- A Network Meta-Analysis On The Effects of Information Technology Application On Preoperative Anxiety of PatientsDocumento7 pagineA Network Meta-Analysis On The Effects of Information Technology Application On Preoperative Anxiety of PatientsInternational Journal of Application or Innovation in Engineering & ManagementNessuna valutazione finora