Potrebbero piacerti anche
- Tugas Health Policy Pak CaliDocumento1 paginaTugas Health Policy Pak CaliAznamryNessuna valutazione finora
- Tugas Health Policy Pak CaliDocumento1 paginaTugas Health Policy Pak CaliAznamryNessuna valutazione finora
- Tugas DonabediDocumento3 pagineTugas DonabediAznamryNessuna valutazione finora
- Creamer Et Al-2016-British Journal of DermatologyDocumento34 pagineCreamer Et Al-2016-British Journal of DermatologyAtika Indah SariNessuna valutazione finora
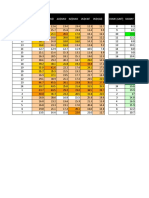
- Hour (GMT +8) Eurusd Gbpusd Audusd Nzdusd Usdchf Usdcad Hour (GMT) UsdjpyDocumento3 pagineHour (GMT +8) Eurusd Gbpusd Audusd Nzdusd Usdchf Usdcad Hour (GMT) UsdjpyAznamryNessuna valutazione finora
- CervicalCancer HPV Feb07Documento24 pagineCervicalCancer HPV Feb07Avicena M IqbalNessuna valutazione finora
- Viruses 02 02493 PDFDocumento16 pagineViruses 02 02493 PDFAznamryNessuna valutazione finora
- Laryngopharyngeal Reflux (Tne)Documento4 pagineLaryngopharyngeal Reflux (Tne)AznamryNessuna valutazione finora
- Final Special Sense Inter FixDocumento15 pagineFinal Special Sense Inter FixAznamryNessuna valutazione finora
- Mikosis Source: THE MERCK MANUAL HOME HEALTH HANDBOOKDocumento1 paginaMikosis Source: THE MERCK MANUAL HOME HEALTH HANDBOOKAznamryNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 1F4 Catalog0808Documento12 pagine1F4 Catalog0808Edwin Ng0% (1)
- Unit Test Nervous System 14.1Documento4 pagineUnit Test Nervous System 14.1ArnelNessuna valutazione finora
- Ragavendhar Seeks Entry Software JobDocumento2 pagineRagavendhar Seeks Entry Software JobfferferfNessuna valutazione finora
- I Am Sharing 'Pregnancy Shady' With YouDocumento48 pagineI Am Sharing 'Pregnancy Shady' With YouNouran AlaaNessuna valutazione finora
- Land-Use PlanningDocumento15 pagineLand-Use PlanningCiara MaryNessuna valutazione finora
- Article 106899Documento6 pagineArticle 106899Abhinave SNessuna valutazione finora
- HV 2Documento80 pagineHV 2Hafiz Mehroz KhanNessuna valutazione finora
- Differentiation SS2Documento88 pagineDifferentiation SS2merezemenike272Nessuna valutazione finora
- Book 2 - Test 1Documento2 pagineBook 2 - Test 1Đức LongNessuna valutazione finora
- Tipolo WH Gantt ChartDocumento15 pagineTipolo WH Gantt ChartMayeterisk RNessuna valutazione finora
- Njhs Application EssayDocumento4 pagineNjhs Application Essaycjawrknbf100% (2)
- List of SQAC DQAC SISC DISC 2019 20Documento39 pagineList of SQAC DQAC SISC DISC 2019 20Shweta jainNessuna valutazione finora
- 2018 Diesel TOYOTA Jun11Documento90 pagine2018 Diesel TOYOTA Jun11eko sulistyo75% (4)
- Product Differentiation and Market Segmentation As Alternative Marketing StrategiesDocumento7 pagineProduct Differentiation and Market Segmentation As Alternative Marketing StrategiesCaertiMNessuna valutazione finora
- Karan Chawla and Joshua Lee November 21, 2016 MEDS 3020 - Fall 2016 Dr. Rosevear, Dr. Cartwright, Dr. LiebermanDocumento2 pagineKaran Chawla and Joshua Lee November 21, 2016 MEDS 3020 - Fall 2016 Dr. Rosevear, Dr. Cartwright, Dr. LiebermanJeremy DelaneyNessuna valutazione finora
- Understanding The Self Metacognitive Reading Report 1Documento2 pagineUnderstanding The Self Metacognitive Reading Report 1Ako Lang toNessuna valutazione finora
- Case Study On Maruti 800Documento4 pagineCase Study On Maruti 800Nizar MesaniNessuna valutazione finora
- VANSINA, Jan. Art History in AfricaDocumento250 pagineVANSINA, Jan. Art History in AfricaRaphaelTim100% (1)
- EVS XT2+ Tech Ref Software Manual v10.03 PDFDocumento80 pagineEVS XT2+ Tech Ref Software Manual v10.03 PDFgibonulNessuna valutazione finora
- Assessing Khazaria-Serpent PeopleDocumento1 paginaAssessing Khazaria-Serpent PeopleJoao JoseNessuna valutazione finora
- Scientific Passage English TestDocumento57 pagineScientific Passage English TestAb HadiNessuna valutazione finora
- Fancy YarnsDocumento7 pagineFancy Yarnsiriarn100% (1)
- Sample ResumeDocumento3 pagineSample Resumeapi-380209683% (6)
- Vernacular Architecture: Bhunga Houses, GujaratDocumento12 pagineVernacular Architecture: Bhunga Houses, GujaratArjun GuptaNessuna valutazione finora
- Chapter 1 Critical Thin...Documento7 pagineChapter 1 Critical Thin...sameh06Nessuna valutazione finora
- Calibration GuideDocumento8 pagineCalibration Guideallwin.c4512iNessuna valutazione finora
- Sr. No. Name Nationality Profession Book Discovery Speciality 1 2 3 4 5 6 Unit 6Documento3 pagineSr. No. Name Nationality Profession Book Discovery Speciality 1 2 3 4 5 6 Unit 6Dashrath KarkiNessuna valutazione finora
- Safety Data Sheet for Instant AdhesiveDocumento6 pagineSafety Data Sheet for Instant AdhesiveDiego S. FreitasNessuna valutazione finora
- Karate Writing AssessmentDocumento2 pagineKarate Writing AssessmentLeeann RandallNessuna valutazione finora
- System Software Module 3: Machine-Dependent Assembler FeaturesDocumento28 pagineSystem Software Module 3: Machine-Dependent Assembler Featuresvidhya_bineeshNessuna valutazione finora