Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Net Work Survey VehicleDocumento26 pagineNet Work Survey VehiclegurvinderkumarNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- (John F. Moulder) PHI Handbook of XRay Photoelectron SpectrosDocumento192 pagine(John F. Moulder) PHI Handbook of XRay Photoelectron SpectrosCamilo CorredorNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Oral Histology & Embryology-FikreDocumento240 pagineOral Histology & Embryology-FikreHeran A AlhadiNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Nested LoopsDocumento11 pagineNested LoopssivaabhilashNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Rpzf2: Product Data SheetDocumento4 pagineRpzf2: Product Data SheetJosé RincónNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Acn CSDocumento4 pagineAcn CSLeo100% (1)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Unit-III - EEFA - CostsDocumento70 pagineUnit-III - EEFA - CostsRamalingam ChandrasekharanNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- High-Strength Stainless Steels With "Microduplex" Structure For Cryogenic ApplicationsDocumento3 pagineHigh-Strength Stainless Steels With "Microduplex" Structure For Cryogenic ApplicationsakhileshNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Part 1Documento120 paginePart 1Raju Halder0% (1)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Role of Virtual Reality Simulation in Surgical Training in The Light of COVID-19 PandemicDocumento13 pagineThe Role of Virtual Reality Simulation in Surgical Training in The Light of COVID-19 PandemicIván Hernández FloresNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Module 3Documento10 pagineModule 3Michael godsonNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- AC Induction Motors - How AC Motors WorkDocumento10 pagineAC Induction Motors - How AC Motors WorkBraulio IrrutiaNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Clipping Clamping CircuitsDocumento7 pagineClipping Clamping CircuitsPavan SaiNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- 8051 Serial CommunicationDocumento35 pagine8051 Serial CommunicationSanthosh CricketNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Upcoming: Advisor Webcast: Oracle Database Resource ManagerDocumento41 pagineUpcoming: Advisor Webcast: Oracle Database Resource ManagerLayne MoránNessuna valutazione finora
- NDT VTL-3-3Documento2 pagineNDT VTL-3-3Priyesh MauryaNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Wood Conserving StovesDocumento117 pagineWood Conserving Stovesalitoparana100% (1)
- Sri Chaitanya: KEY SheetDocumento13 pagineSri Chaitanya: KEY SheetMODALAVALASA SRIHARSHANessuna valutazione finora
- 2016 FSAE Electric Vehicle Pedal Assembly DesignDocumento40 pagine2016 FSAE Electric Vehicle Pedal Assembly Designshubham rastogiNessuna valutazione finora
- Postmodernity in PiDocumento2 paginePostmodernity in Pixhardy27Nessuna valutazione finora
- Assignment 176020307045 PDFDocumento82 pagineAssignment 176020307045 PDFnikita gohelNessuna valutazione finora
- New Model For Predicting Thermal Radiation From Flares and High Pressure Jet Fires For Hydrogen and SyngasDocumento15 pagineNew Model For Predicting Thermal Radiation From Flares and High Pressure Jet Fires For Hydrogen and Syngasthlim19078656Nessuna valutazione finora
- Ec2203-Unit IV Memory Devices Digital ElectronicsDocumento38 pagineEc2203-Unit IV Memory Devices Digital ElectronicsKarthikeyan_Go_952567% (6)
- Python Fundamentals SheetDocumento29 paginePython Fundamentals Sheetwp1barabaNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- TB-2100 Operational and Maintenance Manual Rev C OptimiseDocumento224 pagineTB-2100 Operational and Maintenance Manual Rev C OptimisearnaudmarielNessuna valutazione finora
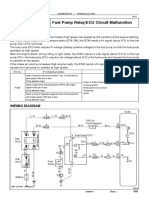
- DTC P1200 Fuel Pump Relay/ECU Circuit MalfunctionDocumento4 pagineDTC P1200 Fuel Pump Relay/ECU Circuit MalfunctiononealNessuna valutazione finora
- Chapter 3 Ni ChupaghettiDocumento2 pagineChapter 3 Ni ChupaghettiRodemar RosarioNessuna valutazione finora
- HVSI804T WGD 83Documento6 pagineHVSI804T WGD 83mnezamiNessuna valutazione finora
- Ubd Planning Template With QuestionsDocumento3 pagineUbd Planning Template With Questionsapi-217297849Nessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Digital - 123328-R010818-Analisa Balik-BibliografiDocumento5 pagineDigital - 123328-R010818-Analisa Balik-BibliografiEncep Septian CaturNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)