Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Step-By-Step Instructions On The: Straumann TibrushDocumento4 pagineStep-By-Step Instructions On The: Straumann Tibrushadambear213Nessuna valutazione finora
- JadaDocumento14 pagineJadaadambear213Nessuna valutazione finora
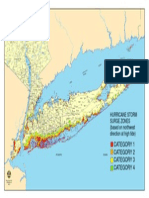
- Nys Storm Surge ZonesDocumento1 paginaNys Storm Surge Zonesadambear213Nessuna valutazione finora
- Periodontal Dictates For Esthetic Ceramometal Crowns: R - Sheldon Stein, DMDDocumento11 paginePeriodontal Dictates For Esthetic Ceramometal Crowns: R - Sheldon Stein, DMDadambear213Nessuna valutazione finora
- 1 ArticlesDocumento2 pagine1 Articlesadambear213Nessuna valutazione finora
- Ideas Academy Reports: and InnovationsDocumento9 pagineIdeas Academy Reports: and Innovationsadambear213Nessuna valutazione finora
- Map ArenaDocumento1 paginaMap Arenaadambear213Nessuna valutazione finora
- OITE Review 2013 TraumaDocumento173 pagineOITE Review 2013 Traumaaddison woodNessuna valutazione finora
- Hemorrhoids InformationDocumento29 pagineHemorrhoids InformationsheilapedzNessuna valutazione finora
- 3 Problems With The Passenger and Powers of LaborDocumento105 pagine3 Problems With The Passenger and Powers of LaborRaquel M. MendozaNessuna valutazione finora
- Facial Plastic and Reconstructive SurgeryDocumento12 pagineFacial Plastic and Reconstructive SurgeryAndrea GuidoteNessuna valutazione finora
- Anatomy and Physiology Vocabulary1Documento10 pagineAnatomy and Physiology Vocabulary1Mobile Legends GamingNessuna valutazione finora
- AnyRidge C4.0Documento80 pagineAnyRidge C4.0Vavi Nichimis100% (1)
- EAU Guidelines Prostate Cancer 2015 v2Documento156 pagineEAU Guidelines Prostate Cancer 2015 v2alaaNessuna valutazione finora
- Obstetric Emergencies PDFDocumento15 pagineObstetric Emergencies PDFEdi BackyNessuna valutazione finora
- Anh Van 3 - Buoi 4 - MAtchingDocumento10 pagineAnh Van 3 - Buoi 4 - MAtchingthi toNessuna valutazione finora
- PhDthesisAASL PDFDocumento168 paginePhDthesisAASL PDFmuhammad alamNessuna valutazione finora
- Catalogue Rudolf - Instrument Surgical - PT. Graha IsmayaDocumento172 pagineCatalogue Rudolf - Instrument Surgical - PT. Graha IsmayayuketamaNessuna valutazione finora
- Medical Disposables: Infusion Disposable ProductsDocumento32 pagineMedical Disposables: Infusion Disposable ProductsKamana ThakurNessuna valutazione finora
- RZ Catalog Urology PDFDocumento75 pagineRZ Catalog Urology PDFrini setyawati50% (2)
- Leadership & Management - Prioritization: Pressure. This Increased NorepinephrineDocumento46 pagineLeadership & Management - Prioritization: Pressure. This Increased NorepinephrineregisterednurseNessuna valutazione finora
- CGHS Rates 2014 - Ahmedabad1Documento51 pagineCGHS Rates 2014 - Ahmedabad1Chirag KoradiaNessuna valutazione finora
- Abdomen AssessmentDocumento9 pagineAbdomen AssessmentAbsalon, J. A. (2201986)Nessuna valutazione finora
- Autogenous - Mineralized - Dentin - Versus - Xenograft - Granules - in - Ridge - Preservation - For Delayed - Implantation - in - Post-Extraction - SitesDocumento11 pagineAutogenous - Mineralized - Dentin - Versus - Xenograft - Granules - in - Ridge - Preservation - For Delayed - Implantation - in - Post-Extraction - SitesSamantha TavaresNessuna valutazione finora
- Bệnh Lý Về Thực QuảnDocumento57 pagineBệnh Lý Về Thực QuảnMai NamNessuna valutazione finora
- Bullous Keratopathy PRDocumento12 pagineBullous Keratopathy PRshevinesaNessuna valutazione finora
- Topik 14. Medical Equipment VocabularyDocumento8 pagineTopik 14. Medical Equipment VocabularyYunita HarahapNessuna valutazione finora
- Higher Education Module ProgramDocumento2 pagineHigher Education Module ProgramWen Jie LauNessuna valutazione finora
- Cerebro NeonatalDocumento8 pagineCerebro NeonatalRodri EspinNessuna valutazione finora
- Hernia: Information For PatientsDocumento2 pagineHernia: Information For Patientsrianrifaldi123_98497Nessuna valutazione finora
- Ati Fundamentals Proctored Exam 20192020 Retake Guide 1Documento27 pagineAti Fundamentals Proctored Exam 20192020 Retake Guide 1muthiimorris68Nessuna valutazione finora
- 2ND Long Exam Week2 Answer Key 1Documento11 pagine2ND Long Exam Week2 Answer Key 1Han NahNessuna valutazione finora
- Bhat - Pediatric TraumaDocumento13 pagineBhat - Pediatric TraumaRicardo GrilloNessuna valutazione finora
- Erythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesDocumento27 pagineErythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesMisbah KaleemNessuna valutazione finora
- A1 5Documento4 pagineA1 5Grace Rabino IINessuna valutazione finora
- Z - SCAPULAR and PARASCAPULAR FLAPDocumento6 pagineZ - SCAPULAR and PARASCAPULAR FLAPTze Yean KongNessuna valutazione finora
- ASSESSING FEMALE MALE GENITALIAS Including The INGUINALDocumento23 pagineASSESSING FEMALE MALE GENITALIAS Including The INGUINALkyla boncacasNessuna valutazione finora