Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Moca B Brazil Pdf1Documento2 pagineMoca B Brazil Pdf1rocolmar100% (1)
- History of Psychology Part Two - The RebirthDocumento73 pagineHistory of Psychology Part Two - The Rebirthrocolmar100% (1)
- Klaus Conrad - History of PsychiatryDocumento20 pagineKlaus Conrad - History of Psychiatryrocolmar100% (1)
- Extra: First Fictional Report of Folie A' DeuxDocumento2 pagineExtra: First Fictional Report of Folie A' DeuxrocolmarNessuna valutazione finora
- Key Concepts in Literary TheoryDocumento209 pagineKey Concepts in Literary Theoryrocolmar100% (2)
- Sulcal, Ventricular, and White Matter Changes at MR Imaging in The Aging Brain: Data From The Cardiovascular Health Study.Documento7 pagineSulcal, Ventricular, and White Matter Changes at MR Imaging in The Aging Brain: Data From The Cardiovascular Health Study.rocolmarNessuna valutazione finora
- A Map For Social Navigation in The Human BrainDocumento14 pagineA Map For Social Navigation in The Human BrainrocolmarNessuna valutazione finora
- The White Matter of The Human Cerebrum - Part I The Occipital Lobe by Heinrich SachsDocumento30 pagineThe White Matter of The Human Cerebrum - Part I The Occipital Lobe by Heinrich SachsrocolmarNessuna valutazione finora
- Norman Geschwind - Selected PapersDocumento566 pagineNorman Geschwind - Selected Papersrocolmar100% (1)
- Visual Agnosia - FarahDocumento207 pagineVisual Agnosia - Farahrocolmar100% (1)
- Philosophy and The PassionsDocumento327 paginePhilosophy and The Passionsrocolmar50% (2)
- Memory Systems of The Brain - A Brief History and Current Perspective LR Squire 2004Documento7 pagineMemory Systems of The Brain - A Brief History and Current Perspective LR Squire 2004rocolmarNessuna valutazione finora
- Diaphragm: Surgical Anatomy of The DiaphragmDocumento14 pagineDiaphragm: Surgical Anatomy of The DiaphragmOlga CerlatNessuna valutazione finora
- 柳奇學姐提供的Mode of Mechanical VentilatorDocumento79 pagine柳奇學姐提供的Mode of Mechanical Ventilatorapi-25944730100% (10)
- Practice Test QuestionsDocumento14 paginePractice Test QuestionsFilipino Nurses CentralNessuna valutazione finora
- Cellular AberrationDocumento2 pagineCellular AberrationFrances Gaviola100% (1)
- Department of Elderly Care: What Is Delirium?Documento2 pagineDepartment of Elderly Care: What Is Delirium?mutiaraNessuna valutazione finora
- Report Study Into The Mental Resilience of Journalists DR Tara SwartDocumento12 pagineReport Study Into The Mental Resilience of Journalists DR Tara SwartfinntheceltNessuna valutazione finora
- Elektrokardiograf: Prof. Dr. Peter KaboDocumento56 pagineElektrokardiograf: Prof. Dr. Peter KaboAchmad DamnhuriNessuna valutazione finora
- Jurnal Rujukan KuesionerDocumento10 pagineJurnal Rujukan KuesionerMiss BerlyantiNessuna valutazione finora
- Oregon V Azar ComplaintDocumento109 pagineOregon V Azar ComplaintHonolulu Star-Advertiser100% (1)
- Clonidine HydrochlorideDocumento1 paginaClonidine HydrochlorideLovelyn Joy Abubo CortezNessuna valutazione finora
- Health Communication and Mass Media CH1 PDFDocumento17 pagineHealth Communication and Mass Media CH1 PDFShamsa KanwalNessuna valutazione finora
- Interproximal Tissue Dimensions in Relation To Adjacent Implants in The Anterior Maxilla - Clinical Observations and Patient Aesthetic EvaluationDocumento11 pagineInterproximal Tissue Dimensions in Relation To Adjacent Implants in The Anterior Maxilla - Clinical Observations and Patient Aesthetic EvaluationEduardo AyubNessuna valutazione finora
- Ret Dem Bed Bath Hair Shampoo WUPDocumento4 pagineRet Dem Bed Bath Hair Shampoo WUPCarissa De Luzuriaga-BalariaNessuna valutazione finora
- What Is Pityriasis Rosea?Documento1 paginaWhat Is Pityriasis Rosea?andinaNessuna valutazione finora
- Notes On Physical Examination of AbdomenDocumento6 pagineNotes On Physical Examination of AbdomenMarwa Al-AzzawiNessuna valutazione finora
- Prepu Psych Chapter 1Documento329 paginePrepu Psych Chapter 1nana100% (1)
- Case PresentationDocumento13 pagineCase Presentationapi-371813266Nessuna valutazione finora
- Psychiatric NursingDocumento32 paginePsychiatric NursingPinky Cuaresma100% (1)
- The Auburn Plainsman 12-3-1998Documento32 pagineThe Auburn Plainsman 12-3-1998The Auburn PlainsmanNessuna valutazione finora
- How To Use Eye Drops ProperlyDocumento9 pagineHow To Use Eye Drops ProperlyQoshrina AdenitaNessuna valutazione finora
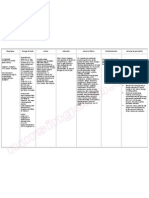
- Cute Baby: Ashroff Memorial Hospital Ward 03Documento27 pagineCute Baby: Ashroff Memorial Hospital Ward 03dhanushkaNessuna valutazione finora
- Impaksi Gigi Molar Tiga BawahDocumento42 pagineImpaksi Gigi Molar Tiga BawahArismunandar SosiloNessuna valutazione finora
- Perspectives On Episodic and Semantic Memory Retrieval. Chaprer 1.1 of The Book Handbook of Episodic Memory.Documento2 paginePerspectives On Episodic and Semantic Memory Retrieval. Chaprer 1.1 of The Book Handbook of Episodic Memory.Tahi GuzmánNessuna valutazione finora
- A Comparative Study of Intrathecal Injection of Bupivacaine Alone or With Fentanyl, Clonidine, and Neostigmine in Lower Abdominal SurgeriesDocumento16 pagineA Comparative Study of Intrathecal Injection of Bupivacaine Alone or With Fentanyl, Clonidine, and Neostigmine in Lower Abdominal SurgeriesdhiyaNessuna valutazione finora
- Acute Renal FailureDocumento15 pagineAcute Renal FailureJoe RealNessuna valutazione finora
- United States Court of Appeals, Second CircuitDocumento9 pagineUnited States Court of Appeals, Second CircuitScribd Government DocsNessuna valutazione finora
- Jaw LashDocumento16 pagineJaw LashSven BivalNessuna valutazione finora
- Shock Syndromes and Sepsis PDFDocumento61 pagineShock Syndromes and Sepsis PDFhuong LNessuna valutazione finora
- Theory of Comfort EnglishDocumento15 pagineTheory of Comfort EnglishedoprimaNessuna valutazione finora
- Listening Sample Test 2 Audio ScriptDocumento12 pagineListening Sample Test 2 Audio ScriptCCCAXANessuna valutazione finora