Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Fulvic Acid Minerals May Prevent Cancer GrowthDocumento42 pagineFulvic Acid Minerals May Prevent Cancer Growthdarlene918Nessuna valutazione finora
- Respiratory SystemDocumento19 pagineRespiratory SystemayuNessuna valutazione finora
- Complete Guide To Urine TheraphyDocumento9 pagineComplete Guide To Urine TheraphyNancy Miro100% (4)
- Taste of Paradise Chapter 4Documento12 pagineTaste of Paradise Chapter 4Gisele Ferreira0% (5)
- PHARMACOTHERAPY OF COUGH SUPPRESSANTS EXPECTORANTS MUCOLYTICSDocumento51 paginePHARMACOTHERAPY OF COUGH SUPPRESSANTS EXPECTORANTS MUCOLYTICSIqra Butt100% (3)
- Health Assessment Handout 3Documento9 pagineHealth Assessment Handout 3ApRil Anne BalanonNessuna valutazione finora
- Assess Head, Eyes, Ears, Nose and ThroatDocumento25 pagineAssess Head, Eyes, Ears, Nose and ThroatApRil Anne BalanonNessuna valutazione finora
- Health Assessment Handout 1Documento9 pagineHealth Assessment Handout 1ApRil Anne BalanonNessuna valutazione finora
- Health Assessment Handout 5Documento10 pagineHealth Assessment Handout 5ApRil Anne BalanonNessuna valutazione finora
- Milestones of Fetal Development PDFDocumento2 pagineMilestones of Fetal Development PDFApRil Anne BalanonNessuna valutazione finora
- Uso de Sustancias en El EmbarazoDocumento9 pagineUso de Sustancias en El EmbarazoDanitza YhovannaNessuna valutazione finora
- STD's EditedDocumento7 pagineSTD's EditedApRil Anne BalanonNessuna valutazione finora
- PBL and Professional LearningDocumento236 paginePBL and Professional LearningApRil Anne BalanonNessuna valutazione finora
- Failure To Thrive JournalDocumento13 pagineFailure To Thrive JournalApRil Anne BalanonNessuna valutazione finora
- Vital Signs Assessment GuideDocumento15 pagineVital Signs Assessment GuideApRil Anne BalanonNessuna valutazione finora
- Heart Disease in Pregnancy ManagementDocumento21 pagineHeart Disease in Pregnancy ManagementS VaibhavNessuna valutazione finora
- Care of The Newborn Care of The NewbornDocumento126 pagineCare of The Newborn Care of The NewbornApRil Anne BalanonNessuna valutazione finora
- Phenylketonuria Congenital HypothyroidismDocumento1 paginaPhenylketonuria Congenital HypothyroidismApRil Anne BalanonNessuna valutazione finora
- Handout 4Documento13 pagineHandout 4ApRil Anne BalanonNessuna valutazione finora
- Handout 1 PDFDocumento3 pagineHandout 1 PDFApRil Anne BalanonNessuna valutazione finora
- Phenylketonuria Congenital HypothyroidismDocumento1 paginaPhenylketonuria Congenital HypothyroidismApRil Anne BalanonNessuna valutazione finora
- Handout 3 PDFDocumento3 pagineHandout 3 PDFApRil Anne BalanonNessuna valutazione finora
- Handout 1 PDFDocumento3 pagineHandout 1 PDFApRil Anne BalanonNessuna valutazione finora
- Gestational Conditions: Hyperemesis Gravidarum Is Severe and Unremitting Nausea or Vomiting Associated WithDocumento13 pagineGestational Conditions: Hyperemesis Gravidarum Is Severe and Unremitting Nausea or Vomiting Associated WithApRil Anne BalanonNessuna valutazione finora
- NCM 109 Handout # 3: GreywolfredDocumento6 pagineNCM 109 Handout # 3: GreywolfredApRil Anne BalanonNessuna valutazione finora
- Handout 4Documento13 pagineHandout 4ApRil Anne BalanonNessuna valutazione finora
- The High-Risk Pregnant Client:: NCM 109 Handout # 1Documento3 pagineThe High-Risk Pregnant Client:: NCM 109 Handout # 1ApRil Anne BalanonNessuna valutazione finora
- Handout 5 PDFDocumento4 pagineHandout 5 PDFApRil Anne BalanonNessuna valutazione finora
- NCM 109 Handout # 2: GreywolfredDocumento3 pagineNCM 109 Handout # 2: GreywolfredApRil Anne BalanonNessuna valutazione finora
- Emotional Support in The Immediate Post Partum 1. Taking PhaseDocumento3 pagineEmotional Support in The Immediate Post Partum 1. Taking PhaseApRil Anne BalanonNessuna valutazione finora
- Greywolfred: NCM 109 Handout # 2Documento4 pagineGreywolfred: NCM 109 Handout # 2ApRil Anne BalanonNessuna valutazione finora
- NCM 109 Handout # 3: GreywolfredDocumento6 pagineNCM 109 Handout # 3: GreywolfredApRil Anne BalanonNessuna valutazione finora
- Handout 4 PDFDocumento3 pagineHandout 4 PDFApRil Anne BalanonNessuna valutazione finora
- Handout 1 PDFDocumento3 pagineHandout 1 PDFApRil Anne BalanonNessuna valutazione finora
- Phenylketonuria Congenital HypothyroidismDocumento1 paginaPhenylketonuria Congenital HypothyroidismApRil Anne BalanonNessuna valutazione finora
- Promoting Activity Tolerance in a Patient with CoughDocumento3 paginePromoting Activity Tolerance in a Patient with CoughitsmeayaNessuna valutazione finora
- Mucinac 600 TabletsDocumento6 pagineMucinac 600 TabletsNurmaNessuna valutazione finora
- Adherence, Anti-Adherence, and Oligosaccharides Preventing Pathogens From Sticking To The Host.Documento61 pagineAdherence, Anti-Adherence, and Oligosaccharides Preventing Pathogens From Sticking To The Host.Didier Alexis Rosales MosqueraNessuna valutazione finora
- Science Reviewer For Science Quiz Elementary: MatterDocumento30 pagineScience Reviewer For Science Quiz Elementary: MatterIan BelgaNessuna valutazione finora
- Frequently Asked Qus (T.me@uworld2021)Documento33 pagineFrequently Asked Qus (T.me@uworld2021)saranya sankarNessuna valutazione finora
- Unit 5 Case StudyDocumento9 pagineUnit 5 Case Studykristin mclaurinNessuna valutazione finora
- About Specific Endonasal Extraction of Cysts of The Maxillary SinusDocumento4 pagineAbout Specific Endonasal Extraction of Cysts of The Maxillary SinusCentral Asian StudiesNessuna valutazione finora
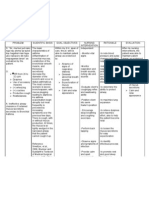
- Cues for Nursing Diagnosis, Pathophysiology, Desired Outcome, Nursing Intervention, Rationale, and Evaluation for DehydrationDocumento3 pagineCues for Nursing Diagnosis, Pathophysiology, Desired Outcome, Nursing Intervention, Rationale, and Evaluation for Dehydrationcheane_jaja67% (3)
- MISTABRON in Bronchopulmonary ObstructionDocumento14 pagineMISTABRON in Bronchopulmonary ObstructionJoyee BasuNessuna valutazione finora
- ENS Guide To Diagnosis & Management (v2 - 09.2016)Documento37 pagineENS Guide To Diagnosis & Management (v2 - 09.2016)Renato Mondani0% (1)
- Ineffective Airway ClearanceDocumento1 paginaIneffective Airway ClearancejomerdalonaNessuna valutazione finora
- URINALYSIS AND HEMATOLOGY LAB RESULTS INTERPRETATIONDocumento4 pagineURINALYSIS AND HEMATOLOGY LAB RESULTS INTERPRETATIONRoxanne Ganayo ClaverNessuna valutazione finora
- Homeopathic Remedy Profile: Natrum MuriaticumDocumento10 pagineHomeopathic Remedy Profile: Natrum MuriaticumvasgarNessuna valutazione finora
- Watts Rousseau Slippery ElmDocumento8 pagineWatts Rousseau Slippery ElmGlowstarNessuna valutazione finora
- Cervical MucusDocumento24 pagineCervical MucusRgn McklNessuna valutazione finora
- Fighting Pneumonia in UgandaDocumento8 pagineFighting Pneumonia in UgandaSuman SowrabhNessuna valutazione finora
- PBL Copd: 1) Mechanics of RespirationDocumento34 paginePBL Copd: 1) Mechanics of RespirationAhmadNessuna valutazione finora
- ASSESSMENT SUBJECTIVE: "Parang Hinang Hina Siya" As Verbalized by TheDocumento4 pagineASSESSMENT SUBJECTIVE: "Parang Hinang Hina Siya" As Verbalized by Thestiffmyster1234Nessuna valutazione finora
- West Et Al. (2009) Probiotics Immunity and ExerciseDocumento20 pagineWest Et Al. (2009) Probiotics Immunity and ExerciseAshley PeartNessuna valutazione finora
- Nasal Delivery of VaccinesDocumento3 pagineNasal Delivery of VaccinesWilfred BakkerNessuna valutazione finora
- Clearing The Air On The Hard Facts of What Smoking Does To Your BodyDocumento5 pagineClearing The Air On The Hard Facts of What Smoking Does To Your BodyIlyana HaniNessuna valutazione finora
- Lesson17 Epithelial CellsDocumento22 pagineLesson17 Epithelial CellsGemma WrigleyNessuna valutazione finora
- Salix Nigra.: Specific Indications.-Sexual Erethism, Irritability, and PassionDocumento39 pagineSalix Nigra.: Specific Indications.-Sexual Erethism, Irritability, and PassionDr Rushen SinghNessuna valutazione finora
- Covid PillDocumento5 pagineCovid PillJustin VallejoNessuna valutazione finora
- Ivy Extracts Effectiveness and Use of An Old Medicinal PlantDocumento9 pagineIvy Extracts Effectiveness and Use of An Old Medicinal PlantSelimHachichaNessuna valutazione finora