S
ince 2008, the USAID Bureau for Global Healths agship
Maternal and Child Health Integrated Program (MCHIP) has
worked in more than 50 developing countries in Africa, Asia, Latin
America and the Caribbean to improve the health of women and their
families. MCHIP supports programming in maternal, newborn and child
health, immunization, family planning, nutrition, malaria and HIV/
AIDS, and encourages opportunities for integration of programs and
services when feasible.
MCHIP addresses the barriers to accessing and using key evidence-based interventions
across the life stagesfrom pre-pregnancy to age 5by linking communities,
primary health facilities and hospitals. By helping countries identify and focus on
those innovations that will save lives, MCHIP supports delivery of evidence-based
interventions through strengthening government health systems, nongovernmental
organizations and other local partners.
MCHIPs overall strategic approach is guided by ve interrelated principles:
Taking high-level impact interventions to scale
Ensuring country ownership
Creating change through global and regional inuence
Improving measurement and use of data at the country and global levels
Expanding coverage through integrated approaches
MCHIP brings together a partnership of organizations with
demonstrated success in reducing maternal and child deaths:
Jhpiego ICF International
John Snow, Inc. (JSI) Broad Branch
Save the Children PSI
PATH JHU/IIP
Introduction
Greater availability of misoprostol enables trained community
health workers to save the lives of women who give birth in areas
that are far from health facilities.
Twenty-ve-year-old Epiphanie felt her labor begin and immediately called
Immanaculee, an MCHIP-trained community health worker who supports the families
in Bugosa village in the Gakenke district of Rwanda, where she lives. Immanaculee
had educated Epiphanie on the importance of making regular prenatal care visits and
encouraged her to deliver at the health center, where she would have access to medicine
and trained providers.
Immanaculee accompanied Epiphanie on the hilly, ve-kilometer trek to the health
center, but the baby would not wait. The health worker quickly found a hidden area
along the way and covered the spot with the colorful cloths that women traditionally
wrap around their waists. There, she helped Epiphanie deliver a healthy baby girl named
Patiente.
Immediately after the baby was born, Immanaculee gave Epiphanie a lifesaving drug
called misoprostol, which she had learned about in her training. When used in the rst
two hours after delivery, misoprostol is highly effective at preventing excessive bleeding
after childbirth, known as postpartum hemorrhage (PPH).
PPH is the leading cause of death among pregnant women globally, and in Rwanda
an astounding 45% of women who perish during childbirth die from PPH. Making
misoprostol available to mothers is particularly important for women in remote areas,
who might have difculty reaching a facility to give birth. Through this Rwandan pilot
programand many other USAID/MCHIP activities being carried out globallymore
than 700,000 women have received this lifesaving medicine.
Epiphanie
O
ver the last two decades, the global community has witnessed
remarkable reductions in the number of maternal deaths
worldwide. Yet, too many women still die in pregnancy and
childbirth from treatable complicationsnearly 800 women per day.
Postpartum hemorrhage (PPH) and pre-eclampsia/eclampsia (PE/E) together account
for more than 40% of maternal deaths. To combat this, MCHIP works in 30 countries
to promote access to lifesaving interventions for pregnant women, and address a
number of areas integral to improving outcomes for mothers and their babies, such as
malaria in pregnancy and care for women affected by HIV. MCHIP provides leadership
and technical assistance at the global and country levels for an integrated package
of interventions to address PPH, PE/E, preterm birth, maternal anemia and other
complications. MCHIP was a key contributor to new World Health Organization
(WHO) recommendations on PPH and PE/E. A critical change advocated by MCHIP was
the provision by lay workers of misoprostol, a lifesaving drug taken immediately after
birth to prevent excessive bleeding.
Many women still give birth at home and MCHIP strives to deliver interventions
that can reach these women. This means that a woman has access to a skilled birth
attendant, as well as the lifesaving drugs she may need. MCHIP recognizes that a skilled
birth attendant, such as a midwife, doctor or nurse, is critical to a safe and successful
delivery. The program works to increase access to these health workers, and has
spearheaded competency-based trainings and development of resources to build provider
skills and condence, not only in maternal health but in essential newborn care and
family planning as well. Respectful Maternity Care is woven into all aspects of MCHIPs
work to strengthen skilled birth attendance.
Quality-of-care studies, conducted in seven countries, and a Multi-Country Analysis
Survey shed light on critical quality-of-care, health system and policy issues, allowing
governments to identify gaps and work toward solutions to prevent and manage the
leading causes of maternal death. Survey results have been used for advocacy at
national and global levels, including contributions to recommendations of the UN
Commission on Life-Saving Commodities.
Maternal Health
I
n spite of existing high-impact interventions for newborn health,
nearly 3 million babies die each year within the rst month of life,
and more than three-quarters of these deaths occur in sub-Saharan
Africa and South Asia. Improvements in the prevention of newborn
death have lagged behind those for maternal and child health.
MCHIP has assisted 37 countries in addressing the three main causes of newborn death:
prematurity, birth asphyxia and infections. There is substantial evidence that the vast
majority of these deaths can be prevented if mothers and newborns receive proven
low-tech solutions.
The program works to expand the use of lifesaving practices and availability of
commodities through global advocacy, collaboration with country leadership, health
worker trainings and system strengthening. In Liberia and Madagascar, for example,
MCHIP collaborated with partners to institute use of chlorhexidine on a babys
umbilical cord at birth for prevention of newborn infections. Bangladesh has also
recently adopted this intervention. This is a simple technology with the potential to
prevent an estimated 500,000 global newborn deaths each year.
MCHIP supports health service providers through training and the development of
resources covering lifesaving practices in newborn care. In Ethiopia, MCHIP helped
standardize newborn health education and supported the training of
24 national trainers and 256 health workers in newborn care including
resuscitation. Over the course of one year, these workers saved the lives
of more than 578 babies who had stopped breathing at birth.
MCHIP recognizes that the sharing of experiences between countries
is essential for adoption and expansion of newborn health services, so
it seeks to create platforms for countries to have the opportunity to
engage in dialogue around maternal and newborn health. In April 2013,
MCHIP and partners hosted the Global Newborn Health Conference
in Johannesburg, South Africa. As a result of this conference, many
countries, including Bangladesh, India, Liberia and Sierra Leone, have
pledged to improve the availability of and access to key neglected interventions such as
Kangaroo Mother Care and the use of antenatal corticosteroids.
Newborn Health
Sixty seconds can mean the difference between life and death for a
newborn who isnt breathing. Thats the window of time a health
care provider has for resuscitation before a baby suffers injury
from lack of oxygen. Jubaida Shirin knows how quickly that
golden minute can tick by.
Jubaida Shirin, a community-based skilled birth attendant in Habiganj District
in Bangladesh, received a call from one of the women she routinely visited during
pregnancy. Minara Khan was in labor. When Shirin arrived at Minaras home, she
examined Minara and found that Minaras baby was in the breech position. She quickly
applied her training to deliver the child, but as she dried and wrapped the infant, she
heard no cries.
The baby girl wasnt breathing.
Shirin put the newborn girl on her left side on the mothers abdomen and tried her
hardest to stimulate the babys breathing by rubbing the skin over her backbone. The
tiny girl did not respond. Shirin next began resuscitating the child using a bag and
mask, just as she had been trained to do. It worked! Her training paid off.
Baby Shifa survived and is
now a healthy toddler.
Jubaida received her
resuscitation training
through a pilot study of the
Helping Babies Breathe
initiative, sponsored by
MCHIP and partners.
Due to the success of
the program and the
strong commitment of the
Bangladeshi government
to womens and childrens
health, training in newborn
resuscitation is now
available across the country. About 1,700 health facilities have been equipped with
resuscitation equipment, and nearly 500 health facilities have received Helping Babies
Breathe training materials. Birth attendants throughout Bangladesh now have the
knowledge and condence to save the lives of babies like Shifa.
Shifa
T
remendous achievements have been made in decreasing the
number of deaths of children under the age of 5. The rate of these
improvements, however, varies greatly from region to region.
In sub-Saharan Africa, for example, 1 in 9 children dies before the
fth birthdaymore than 16 times the average for developed regions.
For Southern Asia, about 1 in 16 children dies before age 5. The good
news is that the primary killers of childrenpneumonia, diarrhea and
malariaare preventable and treatable.
MCHIP has been a vital contributor to the global movement to end preventable child
deaths, working to improve access to lifesaving treatments at both a global and country
levelhaving worked in 17 countries. The program recognizes that efforts to end
preventable child deaths will be successful only when treatment is available to the
populations most at risk. MCHIP has been at the heart of efforts to expand integrated
Community Case Management (iCCM), a strategy to extend the management and care of
childhood illness beyond health facilities. The package addresses diarrhea, pneumonia
and malaria, and is often extended to include newborn health and malnutrition.
Diarrhea and pneumonia have long been the forgotten killers of children under the
age of 5. Through global advocacy, MCHIP has worked with USAID, UNICEF, WHO
and other key partners to refocus global attention on these illnesses and to increase
momentum to address these killers. The development of the Global Action Plan for the
Prevention and Control of Pneumonia and Diarrhea (GAPPD) and the Diarrhea and
Pneumonia Working Group are two examples of this essential shift.
At the country level, MCHIP works to develop child health policies, empower health
workers and ensure that clinicians are trained to accurately identify and manage
childhood illness. In Kenya, for example, MCHIP worked hand-in-hand with national
ministries to reclassify zinc to make it available to treat diarrheal disease without a
prescription and to establish a national plan to introduce iCCM.
A health worker in Mali improves the health of an entire village
by enlisting the help of the community.
Samata village in Mali is a rural, agricultural
community located more than 20 miles from
the nearest health center. Lack of accessible
and high-quality health services was taking
the lives of the children. Villagers would walk
for hours to seek care when their children
were sick.
Toumani Dagno applied for a position
as a community health worker through
the Community Essential Care program,
implemented by MCHIP in collaboration with UNICEF and other partners. He received
training to provide basic health care to the community and was assigned to Samata to
provide treatment to children suffering from diarrhea, malaria and pneumonia.
Toumani quickly became popular in Samata for his kindness and dedication as well as
the quality of the services he provided. In only six months, he treated more than 600 sick
children.
Toumani recognized that he could have an even greater impact by empowering
community members to take care of their own health. He engaged the village authorities
and worked with community women and youth groups to organize educational
campaigns, including the weekly community Day of Safety. With Toumanis
encouragement, the village began promoting proper handwashing and building latrines.
More than a year after Toumani began working in the village, Sidibe Bourama, advisor
to Samatas chief, remarked on the decrease in deaths.
Because of the presence of Toumani, we have not yet registered any child deaths, he
said.There is less travel to the health center to treat children, and this has reduced the
burden on families for the transport and care.
Child Health
Toumani
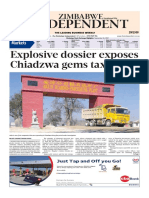
Maternal
Health
Newborn
Health
Child
Health
Malaria
Prevention
& Treatment
Family
Planning
Immunization
Prevention
of HIV/AIDS
An
Integrated
Approach
MCHIP ensures an appropriate mix of
interventions across the life cycle and
along the household-to-hospital
continuum of care. As each partner
takes the lead in developing programs
around a specifc technical area,
MCHIP is able to respond to the needs
for a more integrated approach to
services.
A
n estimated 85% of all deaths from malaria occur in children
under 5. In malaria-endemic areas, 50 million women will become
pregnant each year. These women are highly susceptible to the
consequences of malaria, which lead to increased maternal death and
severe maternal anemia, low birth weight and infant death.
MCHIP works to control malaria, focusing on the prevention and treatment of the
disease among the most vulnerable groupswomen and children in low- and middle-
income countries. The program contributes to global programs and partnerships, most
notably by working with the Roll Back Malaria partnership and the Presidents Malaria
Initiative (PMI).
Through these high-level, global partnerships, MCHIP has helped focus attention on
the importance of addressing MIP, including assisting with the rollout of WHO global
policies regarding MIP prevention and treatment to countries across sub-Saharan
Africa.
At the country level, MCHIP has supported Ministries of Health in 20 African countries
to increase malaria prevention and treatment, integrated with maternal and child
health and HIV programming. Through PMIs Malaria Communities Program, MCHIP
supports efforts of communities and nongovernmental organizations to combat malaria
at the local level.
Because malaria is one of the leading killers of children under the age of 5, MCHIP
strengthens malaria prevention and treatment services for children by working
with countries to introduce and scale up integrated Community Case Management
(iCCM). The iCCM strategy extends lifesaving treatment to children without access to
health facilities by training community health workers in remote villages in the case
management of childhood illness.
By training providers of routine care for pregnant women in
Burkina Faso, the National Malaria Control Program keeps more
women malaria-free during their pregnancy.
Adissa Silga had traveled to the local health clinic for prenatal care and to protect
herself and her unborn child against malaria, a disease endemic to this rural area about
a two-hour drive from Burkina Fasos capital. But the side effects of the chloroquine
pills made her ill and she stopped taking them, which left her at risk of contracting
malaria. Indeed, she later became sick from the disease.
This type of treatment was very hard for me because I often forgot to take my tablets,
Adissa said. Sometimes I avoided taking them because of side effects such as dizziness
and itchiness and, therefore, I contracted malaria and had to stay in the health center
for care. Pregnancies were very hard for me.
Through the MCHIP-supported National Malaria Control Program, Adissa beneted
from an improved prevention regime to help keep her malaria-free during her next
pregnancy. The program works at the national, regional and district levels to build
capacity and strengthen health systems for malaria control and prevention services. The
program pays particular attention to pregnant women and children under the age of 5,
who bear the heaviest burden of malaria.
Each year, approximately 750,000 women in Burkina Faso become pregnant and are at
risk of malaria, which leads to higher rates of maternal anemia and low birth weight
babies. In order to reach more women with interventions to reduce the dangers of
malaria in pregnancy, MCHIP focuses on training the health care providers who see
women during regular antenatal care visits. Since the program began in 2009, MCHIP
has trained health care providers from 17 districts.
Adissa has become a new champion for the program: I can tell you that I feel better. I
would like to encourage each pregnant woman to attend health facilities and that their
pregnancy will be safe and they will have healthy babies.
Malaria Prevention
and Treatment
Adissa
W
orldwide, 222 million women currently wish to delay or prevent
pregnancy, yet do not use contraceptives to plan their family.
The reasons for non-use are complex, involving social, cultural
and economic barriers, fears about side effects and lack of access to a
trusted provider. There is signicant evidence, however, that greater
access to family planning can be vital to achieving global goals in
maternal health and child survival.
MCHIP has helped 21 countries integrate postpartum family planning (PPFP) into
maternal, newborn and child health programming, averting unintended pregnancies
and promoting healthy spacing between pregnancies. MCHIP takes advantage of the
frequent contact women have with health care providers during a pregnancy, birth,
and child health and immunization services to integrate PPFP counseling and services
whenever possible. The program has also developed materials to educate and advocate
for expanded access to the postpartum intrauterine contraceptive device as a reliable
and convenient method of family planning, as well as screening and referral processes to
offer PPFP linked with child health visits.
MCHIP generates and disseminates information on the benets of integrating PPFP
with maternal, newborn and child health services. In Bangladesh, for example, MCHIP
worked with Johns Hopkins University to conduct the Healthy Fertility Study to
examine the effect of an integrated package of services delivered by a female community
health worker on key newborn and infant health practices and use of PPFP to achieve
healthy pregnancy spacing. The studys positive results inuenced other programs in
Bangladesh to adopt the practices, leading to successful scale-up of these practices.
At the global level, MCHIP is a leader in the effort to gather evidence, build consensus,
advocate and innovate around PPFP. An MCHIP-facilitated PPFP Community of
Practice draws attention to the barriers that restrict postpartum womens access to
family planning and tests solutions to address them. MCHIP was an integral partner
with USAID and WHO on the development of the Statement for Collective Action for
Postpartum Family Planning and the forthcoming WHO document on Programming
Strategies for Postpartum Family Planning, garnering global support for PPFP.
An auxiliary nurse-midwife in India educates her community
about options for family planning after birth.
Seema Verma is on a mission. An auxiliary nurse-midwife in Uttarakhand, India,
the mother of two wants to help other women make an informed choice about family
planning services, just as she was able to do.
I want to pass on the same hope and
possibilities to other women in my
community, she said.
When Seema was pregnant for the second
time and looking for a viable, long-term
family planning method, she received
counseling from a visiting team from MCHIP.
They explained the importance of using
contraceptives after delivery to delay or
prevent the next pregnancy. They also gave
her information about the intrauterine contraceptive device (IUCD), which can be
inserted within 48 hours of delivery.
Seema chose to deliver her baby at Womens Hospital in Dehradunan MCHIP
intervention siteso that she could get an IUCD immediately after the birth of her
daughter, Ritika.
For Seema, an IUCD was the best family planning choice for many reasons: It lasts
for 10 years, could be inserted while she was still in the hospital and was free under
government policy. Moreover, she appreciates that she does not need to remember to
take a pill every day.
Seema was so enthusiastic
about her family planning
decision that, while resting
in the postpartum ward, she
counseled two other women
who were sharing the room
with her. They too chose to
have an IUCD inserted. Seema
is optimistic that her decision
offers a promising future for her own two daughters. As one of four children in a poor
family, Seema struggled to nish her schooling and became the most educated member
of her family.
I want my daughters to study more than me, she said. My husband and I want to work
hard to make this possible.
Family Planning
Seema
T
he collaboration of civil society is pivotal to achieving global
aims to end preventable maternal, newborn and child deaths
worldwide. Many international nongovernmental organizations
(iNGOs) and their in-country partners reach underserved and vulnerable
populations with low-cost, high-impact interventions. They are also
often at the forefront of developing practical solutions to the barriers
they encounter on the ground related to implementation and scale-up
of integrated intervention packages to inform national policies and
strategies.
MCHIP supports iNGOs through USAIDs Child Survival and Health Grants Program
(CSHGP)currently 32 projects in 24 countriesthe majority of which involve
partnerships with academia, Ministries of Health and other local entities to implement
and test approaches that bridge gaps in the household-to-health-facility continuum of
the health system.
The MCHIP team provides technical assistance to the grantees in program design,
monitoring, implementation and evaluation, including operations research. This
capacity building promotes a standard level of quality and rigor across projects.
MCHIP also works closely with the CORE Group to foster communities of practice and
contribute to global learning for community health.
Operations research supported through the CSHGP contributes to national and global
evidence. Topics included smart integration of services, civic participation, private-
public partnerships, promoting and advancing equity, community health system
capacity building, and the introduction of low-cost technologies to improve access and
efciency of health interventions.
Grantee work has also been included in recent peer-reviewed publications including:
Health Policy and Planning (February 2013), demonstrating plausible evidence for child
mortality impact, and Global Health: Science and Practice (March 2013), documenting
improvements in under-nutrition at scale in Mozambique, using the Care Group Model.
Catholic Medical Missions Board (CMMB) implemented a Presidents Malaria
Initiative-funded Malaria Communities Program project in three districts of Luapula
Province, Zambia, from 2009 to 2012. Kawambwa, Mwense and Samfya districts are
among those with the highest burden of malaria in the country. Through community
mobilization by community volunteers and traditional leaders, CMMB increased
uptake of malaria prevention and care-seeking and addressed gaps in knowledge and
misconceptions about the use of long-lasting insecticide-treated bed nets (ITNs) and
prevention of malaria in pregnancy.
Just after receiving their award from the Presidents Malaria Initiative (PMI), CMMB
staff joined staff from the 19 other PMI grantees in Nairobi, Kenya, for an MCHIP-
designed and -led training on Program Design, Monitoring, and Evaluation. During the
training, CMMB dened specic project objectives, developed indicators to measure
progress and outcomes, and drafted a monitoring and evaluation plan.
To measure coverage of key interventions and
behaviors and assess project success, CMMB
conducted baseline and endline population-
based coverage surveys. This was the rst time
CMMB had implemented such an exercise in
Zambia. MCHIP worked closely with CMMB
to prepare survey methodology and tools, and
provided on-the-ground training for CMMB
survey enumerators and supervisors. With
the experience gained through the baseline
exercise and ongoing technical assistance
from MCHIP, CMMB was able to conduct
the endline survey independently. CMMB
measured increases in household ITN
ownership, ITN use by children under the age
of 5 and treatment-seeking for children with
fever.
Throughout CMMBs three-year project,
MCHIP reviewed drafts of CMMBs project
work plans, M&E plan and reports to PMI,
providing support and recommendations to strengthen project implementation and
monitoring progress. MCHIP provided technical assistance to 20 NGOs in PMIs
Malaria Communities Program.
Support for Nongovernmental
Organizations, Innovation
and Collaboration
Catholic Medical
Missions Board (PVO/NGO)
G
lobally, immunization prevents 3 million child deaths each year,
and WHO estimates that 17% of the remaining under-5 deaths
approximately 1.5 million deaths annuallycould be prevented
with existing vaccines. Success in reducing vaccine-preventable
mortality has been dramatic, but it cannot be taken for granted.
Achievements in immunization must be maintained and built upon every year. While
infant vaccination coverage in some countries now exceeds 80%, coverage is not the
only measure of success. Before they are exposed to disease, women and newborns must
be reached by both potent vaccines and high-quality services in a timely, safe, effective
and affordable manner so that they return to complete all of their doses. Coverage
disparities also continue within countries, with few countries reaching 80% or higher
coverage in all districts.
MCHIP is dedicated to ensuring that every infant and woman of childbearing age in the
developing world is fully immunized. A great deal of work and planning must take place
behind the scenes before a country can introduce a new lifesaving vaccine. The MCHIP
team applies its technical expertise to support 15 countries through every step of the
introduction process and strengthen routine immunization. When possible, MCHIP
explores opportunities to integrate immunization services with the delivery of other
interventions.
MCHIP programs aim to reach the hard-to-reach and marginalized groups to improve
access, use and equity. The program works with Ministries of Health, civil society
and other partners to identify and prioritize under-immunized populations and
operationalize the Reaching Every District approach.
MCHIP also recognizes that it is important not only to achieve high, countrywide
coverage of each vaccine, but also to ensure that success is sustained even after
coverage goals have been achieved. To prevent outbreaks, uniform and consistently high
coverage is needed everywhere, year after year.
MCHIP works closely with international organizations, such as the GAVI Alliance,
WHO and UNICEF, on important global and regional initiatives. For example, the
program provided technical support to WHO to assist with the response to the pandemic
H1N1 inuenza. MCHIP also serves on many global advisory bodies to use its in-country
experience to inuence immunization policy and strategies.
With meticulous planning and a dedicated staff, the Senegal
Ministry of Health protects the population from meningitis
through a successful vaccine rollout.
In November of 2012, Senegal became the ninth country in the meningitis belta band
of 26 countries stretching from Senegal to Ethiopiato introduce the effective, low-cost
MenAfriVac vaccine through the Meningitis Vaccine Project (MVP), a partnership
between WHO and MCHIP partner PATH. In countries where the vaccine has been
introduced, there has been a dramatic reduction in reported meningitis cases.
The Senegalese Ministry of Health
launched a two-week immunization
campaign in one of the areas of the country
most severely affected by meningitis
outbreaks. Vaccination campaigns
typically target infants under the age of
one, so this project produced a particular
challenge in that it targeted the regions
1- to 29-year-oldsnearly 4 million people.
Organizers needed to take a creative
approach to reach this population by
sending campaign volunteers to the many
places where they would nd young
peopleat work, markets, universities, military camps, prisons, taxi stands, workshops
and in the elds. They traveled by automobiles, bikes, motorcycles and even carts pulled
by donkeys and horses.
MCHIP was a key technical partner in supporting the preparation and implementation
of the campaign. There are many elements that must be planned and considered before
an immunization campaign can even begin, such as public information, staff training,
transportation and distribution logistics, community partnerships, crowd control,
surveillance and planned active monitoring following the campaign to measure the
coverage, quality and impact of the effort.
The launch and distribution of the MenAfriVac vaccine were successful due to the
meticulous organization and careful management of the processes.
Immunization
Senegal Ministry of Health
H
IV is a leading cause of death among women of reproductive age
and a major contributor to maternal mortality in high-prevalence
settings. According to recent estimates, HIV-infected pregnant
or postpartum women have about eight times higher mortality than their
counterparts who are not infected with HIV. Moreover, despite a 24%
drop in new pediatric infections, 900 children are still newly infected
every day.
For the rst time, the global community has the tools needed to virtually eliminate
pediatric HIV and keep HIV-infected women alive and healthy. MCHIP continues to
focus on a strategic approach that
has helped 16 countries scale up
high-impact interventions to prevent
new infections and ensure that HIV-
infected persons are linked to the
care and treatment they need.
To eliminate mother-to-child
transmission of HIV, MCHIP engages
communities to increase access to
services and ensure that women
are utilizing the services. When
and where appropriate, MCHIP
integrates HIV services with other
maternal and newborn health
programs to ensure that women and their families receive the appropriate care they need
for all aspects of their health.
MCHIP is committed to reaching the unreached and underserved populations with
comprehensive HIV services. By adapting the Reaching Every District approach for
prevention of mother-to-child transmission in Kenya, MCHIP and the district health
ofce increased coverage of community health workers in Kenyas Bondo district from
38% to 100% in two years. This led to an improvement in earlier rst antenatal care
visits (from 45% to 76%) as well as labor and delivery coverage in the new facilities (5%
to 15%).
MCHIP has made great strides in the implementation of voluntary medical male
circumcision (VMMC) services, ensuring that the programs are truly country-owned and
integrated within existing health systems. In addition to serving as global advocates for
the intervention, MCHIP has implemented VMMC programs in three countries: Malawi,
Lesotho and Tanzania. As of June 2013, nearly 200,000 MCHIP-supported VMMCs had
been performed.
HIV testing and counseling (HTC) remains a critical gateway to treatment, care and
prevention interventions. MCHIP works with countries to improve HTC systems and
conduct HTC research. In South Sudan, MCHIPs work with 56 health facility staff from
15 facilities meant that staff were trained in testing and counseling; this enabled the
staff to test 4,500 people by January 2013.
Community health workers in Kenya are creating an AIDS-free
generation one pregnancy at a time.
Beatrice and Grace are proof that an AIDS-free generation is within our power. The two
mothers live in the Bondo district in Kenya, where 20% of the community is infected
with HIV, including Beatrice and Grace. Both women, however, gave birth to healthy,
HIV-negative babies thanks to help from community health worker Jane Akoth of the
Barkowino Community Unit.
During their pregnancies, Jane saw Beatrice and Grace regularly, either through home
visits or appointments at the clinic, to ensure that the women were well and their
pregnancies remained healthy.
I like working with these two. They are very good at following advice, said Jane.
Both attended all four of their antenatal clinics and also adhere to their medication.
And both women are grateful for Janes support.
After I delivered my baby, Jane advised me on how to take care of my child by exclusive
breastfeeding for six months and to continue taking my medication, Grace said. I
request Jane to continue doing what she is doing so that she can help other mothers.
Jane is among more than 300 community health workers whose outreach has resulted in
impressive gains. Since 2010, the number of community units under the program more
than doubled, expanding coverage to women living in the most hard-to-reach areas of
Bondo district. As a result, more women are taking advantage of these servicesthe
percentage of expectant mothers going to all four antenatal care visits increased from
25% to 41% in two years, and the percentage of HIV-exposed infants who were tested for
HIV increased from 27% to 78%.
Prevention of HIV/AIDS
Beatrice and Grace
Recognizes that more women and children
will have improved health outcomes if they
have high-quality health services
Values equitable care in all phases of the
work it does to reach the unreached
Increases the impact of tested health care
innovations by taking them to scale
Integrates services, where feasible, to
ensure there are no missed opportunities to
provide care
Provides services within the community
while also maintaining and improving
services at facilities
MCHIP
1300 Pennsylvania Avenue
Washington, DC 20523
tel 202.712.4564
1776 Massachusetts Avenue NW, Suite 300
Washington, DC 20036
tel 202.835.3100
email info@mchip.net
www.mchip.net
Potrebbero piacerti anche
- Donna Vivio USAIDDocumento13 pagineDonna Vivio USAIDMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Dr. Neena Khadka, USAID's Maternal and Child Survival ProgramDocumento18 pagineDr. Neena Khadka, USAID's Maternal and Child Survival ProgramMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Dr. Ziaul Matin, UNICEFDocumento41 pagineDr. Ziaul Matin, UNICEFMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Prof. Shahidullah NBTWC PresentationDocumento39 pagineProf. Shahidullah NBTWC PresentationMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Dr. Bernadette Daelmans, WHO (Day 4)Documento15 pagineDr. Bernadette Daelmans, WHO (Day 4)Maternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Dr. Nigel Livesley, USAID ASSIST ProjectDocumento77 pagineDr. Nigel Livesley, USAID ASSIST ProjectMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Dr. Howard Sobel, WHODocumento50 pagineDr. Howard Sobel, WHOMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- DR Nabila Zaka UNICEF PresentationDocumento15 pagineDR Nabila Zaka UNICEF PresentationMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Summary of Proceedings From The Community Health Worker ForumDocumento22 pagineSummary of Proceedings From The Community Health Worker ForumMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Asia Helping Babies Survive Workshop Agenda 4.5.15Documento6 pagineAsia Helping Babies Survive Workshop Agenda 4.5.15Maternal and Child Survival Program (MCSP)Nessuna valutazione finora
- DR Nalini Singhal AAP PresentationDocumento27 pagineDR Nalini Singhal AAP PresentationMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Helping Babies Survive Agenda 4.5Documento6 pagineHelping Babies Survive Agenda 4.5Maternal and Child Survival Program (MCSP)Nessuna valutazione finora
- DR Bernadette Daelmans WHO PresentationDocumento20 pagineDR Bernadette Daelmans WHO PresentationMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Agenda - Asia Helping Babies Survive WorkshopDocumento6 pagineAgenda - Asia Helping Babies Survive WorkshopMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Infographic: MCHIP Contributions Years 1 - 6Documento1 paginaInfographic: MCHIP Contributions Years 1 - 6Maternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Agenda - Asia Helping Babies Survive WorkshopDocumento6 pagineAgenda - Asia Helping Babies Survive WorkshopMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Summary Report of The Community Health Worker ForumDocumento10 pagineSummary Report of The Community Health Worker ForumMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Quality Session DescriptionDocumento2 pagineQuality Session DescriptionMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Agenda - Asia Helping Babies Survive WorkshopDocumento3 pagineAgenda - Asia Helping Babies Survive WorkshopMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Warner IMPACCT Presentation FinalDocumento12 pagineWarner IMPACCT Presentation FinalSheila LevyNessuna valutazione finora
- Scale Up Map For New Vaccine Introduction in GAVI Supported CountriesDocumento1 paginaScale Up Map For New Vaccine Introduction in GAVI Supported CountriesMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Bottlenecks and Breakthroughs: Lessons Learned From New Vaccine Introductions in Low-Resource Countries, 2008 To 2013Documento44 pagineBottlenecks and Breakthroughs: Lessons Learned From New Vaccine Introductions in Low-Resource Countries, 2008 To 2013Maternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Innovation Vs Sustainability, T. ObothDocumento14 pagineInnovation Vs Sustainability, T. ObothMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Review of Integrated Community Case Management Training and Supervision Materials in Ten African CountriesDocumento71 pagineReview of Integrated Community Case Management Training and Supervision Materials in Ten African CountriesMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Report On The Feasibility of Measuring The iCCM Task Force Indicators Through Existing Monitoring Systems in DRC, Niger, Madagascar, Senegal, South Sudan and ZambiaDocumento37 pagineReport On The Feasibility of Measuring The iCCM Task Force Indicators Through Existing Monitoring Systems in DRC, Niger, Madagascar, Senegal, South Sudan and ZambiaMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Community Session DescriptionDocumento2 pagineCommunity Session DescriptionMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Emerging Ideas From MCHIP Immunization Workshop, Harare, ZimbabweDocumento2 pagineEmerging Ideas From MCHIP Immunization Workshop, Harare, ZimbabweMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Quality of Antenatal and Delivery Care Services in Six Countries in Sub-Saharan AfricaDocumento10 pagineQuality of Antenatal and Delivery Care Services in Six Countries in Sub-Saharan AfricaMaternal and Child Survival Program (MCSP)Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Case Study 07 GlaxoSmithKline VirtueDocumento2 pagineCase Study 07 GlaxoSmithKline VirtueCorina MarinicăNessuna valutazione finora
- DiseasesDocumento150 pagineDiseasessandip nagareNessuna valutazione finora
- White Et Al-2018-Malaria JournalDocumento12 pagineWhite Et Al-2018-Malaria JournalGraciela MezaNessuna valutazione finora
- SVLT Lab Report DetailsDocumento2 pagineSVLT Lab Report Detailsaman.dubey.resNessuna valutazione finora
- IMCIDocumento27 pagineIMCImesdejen100% (6)
- Questions and Answers IMCIDocumento13 pagineQuestions and Answers IMCIEmvie Loyd Pagunsan-Itable100% (10)
- IMCI Chart 2014 EditionDocumento80 pagineIMCI Chart 2014 EditionHarold DiasanaNessuna valutazione finora
- East Africa Climate Change Impacts Final 2Documento12 pagineEast Africa Climate Change Impacts Final 2theone1998Nessuna valutazione finora
- Infectious Disease in An Era of GlobalDocumento13 pagineInfectious Disease in An Era of Globalsebastian herreraNessuna valutazione finora
- Fever Proforma and Assignment - 1Documento48 pagineFever Proforma and Assignment - 1SivaNessuna valutazione finora
- Plan and Fund Health ProjectsDocumento5 paginePlan and Fund Health Projectscarolsmith1957Nessuna valutazione finora
- Peace Corps Mali Welcome Book - October 2011Documento94 paginePeace Corps Mali Welcome Book - October 2011Accessible Journal Media: Peace Corps DocumentsNessuna valutazione finora
- UntitledfhhDocumento40 pagineUntitledfhhMichaelNessuna valutazione finora
- Mukerji Committee Report 1966Documento47 pagineMukerji Committee Report 1966lalit823187100% (1)
- WHR 5 99 - en Malaria Tobacco New Dis Persistent Prob H SystDocumento136 pagineWHR 5 99 - en Malaria Tobacco New Dis Persistent Prob H Systkareem79Nessuna valutazione finora
- Amref's Annual Report For Year Two of The Katine ProjectDocumento23 pagineAmref's Annual Report For Year Two of The Katine ProjectLizFordNessuna valutazione finora
- Vishamajwaram Kc029gdg 121226100307 Phpapp02Documento238 pagineVishamajwaram Kc029gdg 121226100307 Phpapp02Samhitha Ayurvedic Chennai100% (2)
- Identifying Mosquitocidal Compounds from Calendula arvensisDocumento8 pagineIdentifying Mosquitocidal Compounds from Calendula arvensisMalik Ijaz Khan100% (1)
- LGU Scorecard On Health-DILG 2014Documento16 pagineLGU Scorecard On Health-DILG 2014JoEd VillAlonNessuna valutazione finora
- ISLA MIMAROPA - First IssueDocumento20 pagineISLA MIMAROPA - First IssueLester AnonuevoNessuna valutazione finora
- q3 - Week1 - Health 10 - Study ConceptDocumento2 pagineq3 - Week1 - Health 10 - Study ConceptDhess Mulleda MantalaNessuna valutazione finora
- Cause & Pathophysiology of MalariaDocumento8 pagineCause & Pathophysiology of MalariaMariam Mohamed RagehNessuna valutazione finora
- Malaria Prevention 1Documento3 pagineMalaria Prevention 1Anastasia Caesarani KristelNessuna valutazione finora
- (Advances in Parasitology 31) J.R. Baker and R. Muller (Eds.) - Academic Press (1992) PDFDocumento447 pagine(Advances in Parasitology 31) J.R. Baker and R. Muller (Eds.) - Academic Press (1992) PDFStoian GoranovNessuna valutazione finora
- Role of Hospitals in DisastersDocumento3 pagineRole of Hospitals in Disasterssanjay yadavNessuna valutazione finora
- University of Shendi Faculty of Medicine and Surgery OSCE GuideDocumento35 pagineUniversity of Shendi Faculty of Medicine and Surgery OSCE GuideYassin Jamal67% (3)
- Proceedings: Pusat Unggulan IPTEKS (PUI-P2PTM) Poltekkes Kemenkes Semarang 2021 ISBN: 978-623-5709-13-0Documento18 pagineProceedings: Pusat Unggulan IPTEKS (PUI-P2PTM) Poltekkes Kemenkes Semarang 2021 ISBN: 978-623-5709-13-0JVI SambuagaNessuna valutazione finora
- Dwnload Full Managerial Economics 4th Edition Froeb Test Bank PDFDocumento35 pagineDwnload Full Managerial Economics 4th Edition Froeb Test Bank PDFentotic.bathetic8ttq100% (10)
- Mosquito Repellent Activity of Phytochemical ExtractsDocumento6 pagineMosquito Repellent Activity of Phytochemical ExtractsYutaNessuna valutazione finora
- Types and Effects of Water PollutionDocumento44 pagineTypes and Effects of Water PollutionLuqman NHNessuna valutazione finora