Potrebbero piacerti anche
- Future E-Waste ScenariosDocumento19 pagineFuture E-Waste Scenariosmariiusssica2008Nessuna valutazione finora
- TBCDocumento3 pagineTBCwenyinriantoNessuna valutazione finora
- Future E-Waste ScenariosDocumento19 pagineFuture E-Waste Scenariosmariiusssica2008Nessuna valutazione finora
- Opti 755 TechspecsDocumento45 pagineOpti 755 TechspecsPlacidus DsilvaNessuna valutazione finora
- Colombia Highlights Spanish Web PDFDocumento16 pagineColombia Highlights Spanish Web PDFFelipe Murillo AriasNessuna valutazione finora
- Logo 2Documento1 paginaLogo 2Felipe Murillo AriasNessuna valutazione finora
- Enflis ClapDocumento1 paginaEnflis ClapFelipe Murillo AriasNessuna valutazione finora
- 1 s2.0 S2319417016000093 MainDocumento7 pagine1 s2.0 S2319417016000093 MainFelipe Murillo AriasNessuna valutazione finora
- Actualizacion en Hipertension Pulmonar 2013 JaccDocumento13 pagineActualizacion en Hipertension Pulmonar 2013 JaccFelipe Murillo AriasNessuna valutazione finora
- Lo Mejor ArcgisDocumento190 pagineLo Mejor ArcgisFelipe Murillo AriasNessuna valutazione finora
- Acv Hemorragico Lancet 2009Documento25 pagineAcv Hemorragico Lancet 2009Felipe Murillo AriasNessuna valutazione finora
- Clase 3-Distribucion FasesDocumento41 pagineClase 3-Distribucion FasesFelipe Murillo AriasNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Jurnal 2Documento8 pagineJurnal 2AnggunbokingsNessuna valutazione finora
- GMMMC Sukkur MbbsDocumento6 pagineGMMMC Sukkur MbbsSherazAhmedNessuna valutazione finora
- Helping Psychiatry Residents Cope With Patient SuicideDocumento5 pagineHelping Psychiatry Residents Cope With Patient SuicidedrguillermomedinaNessuna valutazione finora
- Hospitalization and Its Effect For Patient - UNTAD 2011 PDFDocumento26 pagineHospitalization and Its Effect For Patient - UNTAD 2011 PDFRiris SutrisnoNessuna valutazione finora
- Special Round Seats For MD - MS - Diploma & DNB SeatsDocumento23 pagineSpecial Round Seats For MD - MS - Diploma & DNB SeatsManoj KashyapNessuna valutazione finora
- Revision Notes On FRCRDocumento385 pagineRevision Notes On FRCRObaidy Albushaher100% (2)
- Acetaminophen (Paracetamol, Tylenol, Tempra, Panadol)Documento3 pagineAcetaminophen (Paracetamol, Tylenol, Tempra, Panadol)Jocelyn Rivera0% (1)
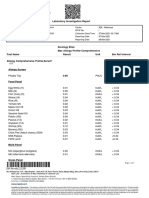
- Case Report: Hepatitis BDocumento34 pagineCase Report: Hepatitis Bdewi sartikaNessuna valutazione finora
- Law Exam NotesDocumento11 pagineLaw Exam NotesEric Cheng100% (1)
- Notes On MRI - FinalDocumento16 pagineNotes On MRI - FinalAnju GuptaNessuna valutazione finora
- Dietary Supplements and Functional Foods 2 Sides of A Coin PDFDocumento7 pagineDietary Supplements and Functional Foods 2 Sides of A Coin PDFNoor FadhilaNessuna valutazione finora
- JednjakDocumento15 pagineJednjakbojana1994Nessuna valutazione finora
- 1st Floor No 105 Above Raymonds Opp Medical College Koti: SHARMA Bpo SupportDocumento4 pagine1st Floor No 105 Above Raymonds Opp Medical College Koti: SHARMA Bpo SupportMK Musthafa GudalurNessuna valutazione finora
- Cardiac MarkersDocumento23 pagineCardiac Markerssulastri triNessuna valutazione finora
- BeraDocumento20 pagineBeraMuhamad SyaifulNessuna valutazione finora
- Laboratory Investigation ReportDocumento7 pagineLaboratory Investigation ReportAmarjeetNessuna valutazione finora
- Head Nurse Experience (Staffing)Documento3 pagineHead Nurse Experience (Staffing)Abigail BrillantesNessuna valutazione finora
- Vascular DementiaDocumento8 pagineVascular Dementiaddelindaaa100% (1)
- Tetanus and Tetanus ToxoidDocumento24 pagineTetanus and Tetanus ToxoidFikar MajidNessuna valutazione finora
- Optic Nerve Glioma: Case Series With Review of Clinical, Radiologic, Molecular, and Histopathologic CharacteristicsDocumento5 pagineOptic Nerve Glioma: Case Series With Review of Clinical, Radiologic, Molecular, and Histopathologic CharacteristicsUtama Hadiputra SurbaktiNessuna valutazione finora
- How To Prepare For ExamDocumento4 pagineHow To Prepare For ExamJaspreet KaurNessuna valutazione finora
- Test Bank For Phlebotomy 4th Edition by Warekois DownloadDocumento9 pagineTest Bank For Phlebotomy 4th Edition by Warekois Downloadryanparker18011988fno100% (23)
- Rich Picture Blood BankDocumento3 pagineRich Picture Blood Bankviannyzerlinda50% (2)
- Management of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesDocumento7 pagineManagement of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesdaypranitaNessuna valutazione finora
- Muir's Textbook of Pathology 15e KulitDocumento35 pagineMuir's Textbook of Pathology 15e Kulitputri theresiaNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaErick PrasetyaNessuna valutazione finora
- The Cracked Mirror, Karen KernbergDocumento10 pagineThe Cracked Mirror, Karen Kernbergjuaromer100% (1)
- Female Sexual DysfunctionDocumento18 pagineFemale Sexual DysfunctionRisky SetiawanNessuna valutazione finora
- AAPM-TG53 (Quality Assurance For Clinical RTP)Documento57 pagineAAPM-TG53 (Quality Assurance For Clinical RTP)ΜΡ_Nessuna valutazione finora
- 5 - Formal ReportDocumento16 pagine5 - Formal ReportJacob MarczakNessuna valutazione finora