Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Metacognition, and Risk Behavior
Caricato da
1195680 valutazioniIl 0% ha trovato utile questo documento (0 voti)
31 visualizzazioni10 pagineStudy explores 2 key variables in social metacognition: perceived intelligence and perceived levels of knowledge about a specific content domain. Higher levels of perceived intelligence at wave 1 were associated with a lower probability of the occurrence of a pregnancy over the ensuing year.
Descrizione originale:
Titolo originale
Metacognition, And Risk Behavior
Copyright
© © All Rights Reserved
Formati disponibili
PDF, TXT o leggi online da Scribd
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoStudy explores 2 key variables in social metacognition: perceived intelligence and perceived levels of knowledge about a specific content domain. Higher levels of perceived intelligence at wave 1 were associated with a lower probability of the occurrence of a pregnancy over the ensuing year.
Copyright:
© All Rights Reserved
Formati disponibili
Scarica in formato PDF, TXT o leggi online su Scribd
0 valutazioniIl 0% ha trovato utile questo documento (0 voti)
31 visualizzazioni10 pagineMetacognition, and Risk Behavior
Caricato da
119568Study explores 2 key variables in social metacognition: perceived intelligence and perceived levels of knowledge about a specific content domain. Higher levels of perceived intelligence at wave 1 were associated with a lower probability of the occurrence of a pregnancy over the ensuing year.
Copyright:
© All Rights Reserved
Formati disponibili
Scarica in formato PDF, TXT o leggi online su Scribd
Sei sulla pagina 1di 10
Metacognition, Risk Behavior, and Risk Outcomes: The Role of Perceived
Intelligence and Perceived Knowledge
James Jaccard and Tonya Dodge
University at Albany, State University of New York
Vincent Guilamo-Ramos
Columbia University
The present study explores 2 key variables in social metacognition: perceived intelligence and perceived
levels of knowledge about a specific content domain. The former represents a judgment of ones
knowledge at an abstract level, whereas the latter represents a judgment of ones knowledge in a specific
content domain. Data from interviews of approximately 8,411 female adolescents from a national sample
were analyzed in a 2-wave panel design with a year between assessments. Higher levels of perceived
intelligence at Wave 1 were associated with a lower probability of the occurrence of a pregnancy over
the ensuing year independent of actual IQ, self-esteem, and academic aspirations. Higher levels of
perceived knowledge about the accurate use of birth control were associated with a higher probability of
the occurrence of a pregnancy independent of actual knowledge about accurate use, perceived intelli-
gence, self-esteem, and academic aspirations.
Keywords: IQ, intelligence, risk behavior, adolescence
There is a growing body of literature in psychology on meta-
cognition and the processes involved in knowing what we know
(e.g., Metcalfe & Shimamura, 1994; Nelson, 1992). Most of this
research has evolved from developmental psychology and cogni-
tive psychology. Developmental psychologists have examined
childrens perceptions of what they know, typically in the form of
competence and ability judgments, and how these judgments
change as a function of age (e.g., Ruble, Boggiano, Feldman, &
Loebl, 1980; Ruffman & Olson, 1989; Stipek & MacIver, 1989;
Wimmer, Hogrefe, & Perner, 1988). Cognitive psychologists have
focused on metainference with respect to lack of knowledge (Gen-
tner & Collins, 1981), illusions of knowing (Epstein, Glenberg, &
Bradley, 1984; Glenberg, Wilkinson, & Epstein, 1982), overcon-
fidence in probability calibrations (Keren, 1991), and the bases of
do not know responses to test questions (Glucksberg & McClos-
key, 1981; Kolers & Palef, 1976). In addition, studies have exam-
ined the feeling-of-knowing phenomenon and how this affects
learning in memory experiments (e.g., Nelson, Gerler, & Narens,
1984; Schacter, 1983; Strack & Forester, 1999).
More recently, psychologists have turned their attention to meta-
cognition in the social domain (Jost, Kruglanski, & Nelson, 1999;
Kruger & Dunning, 1999; Nelson, Kruglanski, & Jost, 1998;
Yzerbyt & Lories, 1999). The present research draws on the recent
metacognitive movement in psychology to explore two key vari-
ables in metacognition as they relate to the prediction of adolescent
health risk behavior. The first variable is perceived intelligence,
which represents a judgment of ones mental intellect and breadth
of knowledge at an abstract level. The second variable is perceived
knowledge, which represents a judgment of ones knowledge about
a specific content domain (e.g., knowledge about birth control or
alcohol). These metacognitions are important because they may
impact behavior independent of actual intelligence and actual
knowledge. The present study describes competing psychological
models relating these constructs to risk behavior and risk out-
comes, empirically evaluates these models, and elucidates the
dynamics by which perceived intelligence at the abstract level may
coalesce with perceived knowledge at the specific level to impact
risk behavior. In so doing, the research extends core constructs in
metacognition to the analysis of health risk behavior.
Perceived Intelligence and Risk Behavior
There is a large body of literature in psychology on constructs
related to perceived intelligence. These include, for example, the
construct of self-efficacy, which focuses on peoples judgments of
their ability to perform certain behaviors (Bandura, 1986, 1989),
James Jaccard and Tonya Dodge, Department of Psychology, University
at Albany, State University of New York; Vincent Guilamo-Ramos, School
of Social Work and Heilbrunn Department of Population and Family
Health, Mailman School of Public Health, Columbia University.
Tonya Dodge is now at the Department of Psychology, George Wash-
ington University.
This research is based on data from the Add Health project, a program
project designed by J. Richard Udry (Principal Investigator) and Peter
Bearman and funded by National Institute of Child Health and Human
Development Grant P01-HD31921 to the Carolina Population Center,
University of North Carolina at Chapel Hill, with cooperative funding
participation by the National Cancer Institute; the National Institute of
Alcohol Abuse and Alcoholism; the National Institute on Deafness and
Other Communication Disorders; the National Institute of Drug Abuse; the
National Institute of General Medical Sciences; the National Institute of
Mental Health; the National Institute of Nursing Research; the Office of
AIDS Research, National Institutes of Health (NIH); the Office of Behav-
ior and Social Science Research, NIH; the Office of the Director, NIH; the
Office of Research on Womens Health, NIH; the Office of Population
Affairs, Department of Health and Human Services (HHS); the National
Center for Health Statistics, Centers for Disease Control and Prevention,
HHS; the Office of Minority Health, Centers for Disease Control and
Prevention, HHS; the Office of Minority Health, Office of Public Health
and Science, HHS; the Office of the Assistant Secretary for Planning and
Evaluation, HHS; and the National Science Foundation.
Correspondence concerning this article should be addressed to James
Jaccard, who is now at the Department of Psychology, Florida International
University, University Park, Miami, FL 33199. E-mail: jjaccard@fiu.edu
Health Psychology Copyright 2005 by the American Psychological Association
2005, Vol. 24, No. 2, 161170 0278-6133/05/$12.00 DOI: 10.1037/0278-6133.24.2.161
161
and attribution theory, which examines how failure on easy or
difficult tasks influences judgments of ability, self-esteem, and
future task performance (e.g., Weiner, 1994; Weiner, Russell, &
Lerman, 1979). Despite this, the construct of perceived intelli-
gence itself, namely how intelligent a person perceives himself or
herself to be, has been studied with much less frequency. Per-
ceived intelligence is potentially important because it represents a
broad-based ability judgment that can serve as a foundation for
inferences about more specific abilities (e.g., Parsons, 1983; Wood
& Bandura, 1989). In addition, perceived intelligence has been
shown to be predictive of important behaviors in the achievement
domain (e.g., Bailey, 1971; Bailey & Mettetal, 1977; Lent, Brown,
& Larkin, 1984).
The present research evaluates three different causal models
linking perceived intelligence to negative risk outcomes in adoles-
cents. Each model includes actual IQ in the theoretical system. The
first model, called the spurious effect model, views the association
between perceived intelligence and risk outcome as spurious in
nature and lacking theoretical import. According to this model,
judgments of self-intelligence are based, in part, on the many
experiences of success and failure that an individual incurs over
the course of life. To the extent that actual IQ influences the
occurrence of these successfailure experiences, a correlation be-
tween perceived intelligence and actual IQ is expected. Indeed,
small to moderate correlations between these constructs have been
reported in previous research (e.g., Bailey & Mettetal, 1977;
Gabriel, Critelli, & Ee, 1994). Cliquet and Balcaen (1983) and
Mott (1983) reported inverse relations between measures of IQ and
sexual risk-taking behavior. IQ scores also have been found to be
negatively related to delinquency and truancy (e.g., Moffit, Gab-
rielli, Mednick, & Schulsinger, 1981). If perceived intelligence is
positively correlated with ones IQ and risk behavior is inversely
correlated with IQ, then one might also expect an inverse relation-
ship between perceived intelligence and risk behavior because of
the common cause of IQ on both constructs. This is the essence of
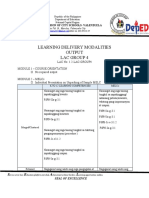
the spurious effect model, illustrated in Figure 1a.
The second model, called the independent effects model, rec-
ognizes that part of the association between perceived intelligence
and risk behavior is spurious (because of the common cause of IQ),
but the model also asserts that perceived intelligence has indepen-
dent effects on risk behavior (see Figure 1b). There are several
mechanisms by which perceived intelligence may have indepen-
dent effects on risk behavior. First, individuals who perceive
themselves as being intelligent may have higher levels of self-
esteem, and this, in turn, may serve as a protective factor vis-a`-vis
risk behavior. For example, a number of studies have found
self-esteem to be negatively associated with sexual risk taking,
alcohol use, smoking, and drug use (e.g., Jang & Thornberry,
1998; Oetting, Deffenbacher, & Donnermeyer, 1998; Pederson,
Koval, McGrady, & Tyas, 1998). Second, those who believe they
are of higher intelligence may have higher academic aspirations,
and such aspirations may decrease the likelihood of risk behavior.
It is well known that adolescents with high academic aspirations
and who do well in school are less prone to engage in a wide
variety of risk behaviors, such as smoking, drinking, unprotected
sex, and drug use (e.g., Griffin, Botvin, Doyle, Diaz, & Epstein,
1999; Jessor, Costa, Jessor, & Donovan, 1983; Kasen, Cohen, &
Brook, 1997; Mott, 1983; Raine, Jenkins, Aarons, Woodward, &
Fairfax, 1999). It seems logical that those who believe themselves
to be more intelligent than others also may have more lofty
academic aspirations, thereby lowering the probability of engaging
in risk behaviors that threaten those aspirations. The present re-
search tests this independent effects model and evaluates the
possible mediating roles of self-esteem and academic aspirations.
The third model, called the mediation model, assumes that
perceived intelligence is the primary determinant of risk behavior
(with those who perceive themselves as intelligent being less likely
to engage in risk behavior) and that this construct, in turn, mediates
the impact of IQ on risk behavior. IQ influences risk behavior, but
it does so only because of its influence on perceived IQ.
The three models of Figure 1 can be differentiated empirically
on the basis of competing predictions about partial coefficients in
the context of regression analysis or structural equation modeling.
One purpose of the present research was to test these models.
Perceived Knowledge and Risk Behavior
Perceived intelligence represents individuals characterizations
of their mental abilities and knowledge at a general level. People
also have perceptions of how knowledgeable they are about spe-
cific content domains, and these judgments may, in turn, impact
their risk behavior in that domain independent of their actual
knowledge. A common finding in studies of confidence and test
performance is a weak association between confidence in perfor-
mance and actual performance, with individuals showing a ten-
dency to be overconfident in their ability to provide correct an-
swers (e.g., Lichenstein & Fischoff, 1977; Quadrel, Fischoff, &
Davis, 1993; Radecki & Jaccard, 1995). Kruger and Dunning
(1999) found that individuals with lower levels of actual knowl-
edge tended to overestimate their ability levels more than did those
individuals with higher levels of actual knowledge. In addition,
individuals with lower levels of actual knowledge were limited in
their ability to recognize competence in others. These studies, as
well as others, suggest that perceptions of how knowledgeable one
is about a specific content domain may have only weak correspon-
dence with ones actual knowledge in that domain.
Few theorists have explored the relationship between perceived
knowledge and risk behavior or risk outcomes. In one of the few
relevant studies we could locate, Quadrel et al. (1993) identified
low-risk and high-risk adolescents and found that at-risk adoles-
cents had higher levels of confidence and lower levels of knowl-
edge than did low-risk adolescents on questions about HIV, preg-
nancy, alcohol use, and drug use. Unfortunately, this study was
limited because the knowledge items used for the two groups were
different, thereby obscuring the results. The present study exam-
ined the issue more directly.
There are many types of knowledge relevant to risk behavior,
but one type that is particularly important is knowledge that helps
one avoid the negative consequences that can result from risk
behavior. For example, knowledge about the accurate use of birth
control methods represents knowledge that helps one prevent the
occurrence of an unintended pregnancy. Knowledge about what
constitutes light, moderate, or heavy alcohol consumption is
knowledge that may prevent one from ultimately developing a
drinking problem, as one monitors ones drinking behavior and
maintains an acceptably light consumption regimen. The conse-
quences of misperceptions of this type of knowledge, we hypoth-
esize, should depend on ones actual knowledge. When actual
knowledge is low, higher levels of perceived knowledge tend to
162
JACCARD, DODGE, AND GUILAMO-RAMOS
represent increasingly erroneous overestimations about ones
knowledge base. In this case, individuals think they know how to
protect themselves against the adverse consequences of a risk
behavior when, in fact, they do not. Such individuals should be at
a higher risk of experiencing negative outcomes as a result of that
risk behavior, everything else being equal. By contrast, when
actual knowledge levels are high, variations in perceived knowl-
edge tend to reflect differing tendencies to underestimate ones
knowledge base. Such underestimations probably will be inconse-
quential in terms of the individuals ability to effectively avoid the
adverse consequences of a risk behavior because the individual has
the knowledge base to do so, independent of his or her perceptions.
Another purpose of the present study was to test this
conceptualization.
An alternative model relating perceived knowledge to risk be-
havior is plausible. This model holds that higher levels of per-
ceived knowledge lead to a higher probability of suffering risk
consequences independent of actual knowledge. According to this
formulation, individuals who believe they are knowledgeable
about how to avoid the adverse consequences of a risk behavior are
more likely to engage in risk behaviors because they believe that
they have the requisite knowledge to avoid the adverse conse-
quences of that behavior. In reality, these individuals are no more
likely than others to have such knowledge (because of the rela-
tively low correlation between perceived knowledge and actual
knowledge), and as a result, the individuals with higher levels of
perceived knowledge will be more likely to experience the adverse
effects of the risk behavior by virtue of the fact that they are
engaging in it more often than others. The present study also
evaluated this model.
Figure 1. Three models of the relationship among perceived intelligence, intelligence, and risk behavior. a:
Spurious effect model. b: Independent effects model. c: Mediation model.
163
METACOGNITION, RISK BEHAVIOR, AND RISK OUTCOMES
The Relationship Between Perceived Intelligence and
Perceived Knowledge
We could locate no study that has examined the relationship
between perceived intelligence and perceived knowledge in a
given risk domain. Nor could we locate research that has examined
the joint influence of the two constructs on risk outcomes. One
possible prediction about the relationship of perceived intelligence
to perceived knowledge in a specific domain is that the two
constructs should be positively correlated. For example, judgments
of higher levels of perceived intelligence may produce a halo
effect (Anderson, 1981) that disposes people to overestimate their
knowledge relative to their actual knowledge in specific content
domains. If individuals think that they are knowledgeable and
smart in general, then they may tend to think of themselves as
knowledgeable in specific content domains. An alternative possi-
bility is that individuals with higher levels of perceived intelli-
gence may be less defensive about their lack of knowledge in a
specific content domain and, hence, be more willing to admit their
ignorance. This, in turn, would lead them to report, and perhaps
actually believe, that they have lower levels of perceived knowl-
edge as they show a greater appreciation for the complexity of the
world. Individuals with low levels of perceived intelligence, by
contrast, may be more defensive about admitting their lack of
knowledge and therefore report and actually believe that they have
higher levels of perceived knowledge in a given content domain.
The defensiveness model makes predictions opposite to the halo-
effect model, with the former predicting an inverse relationship
between perceived intelligence and perceived knowledge and the
latter predicting a direct relationship between perceived intelli-
gence and perceived knowledge. Another purpose of the present
study was to test these competing predictions.
In sum, there has been a great deal of attention in psychology to
metacognition and processes involved in metacognition. Most of
this research has been conducted in cognitive and developmental
psychology, although the constructs have started to emerge in
health psychology. Perceived knowledge about a given content
domain represents metacognition at a concrete, specific level,
whereas perceived intelligence represents metacognition at a more
abstract, general level. Both levels of metacognition may be re-
lated to risk behavior. The present study tests several models of the
relationship between these variables and risk outcomes. Specifi-
cally, the theoretical mechanisms were tested in the context of a
longitudinal study by using a nationally representative sample of
female adolescents to predict the occurrence of a pregnancy. The
knowledge constructs focused on actual and perceived knowledge
about how to appropriately use contraception to avoid a pregnancy.
Method
Overview
The study used a two-wave longitudinal design to predict the occurrence
of a pregnancy between the two waves of assessment. Measures of per-
ceived intelligence, IQ, perceived knowledge about the accurate use of
birth control, and actual knowledge about the accurate use of birth control
as measured at Wave 1 of the survey were the primary predictor variables.
Respondents
The analysis used the National Longitudinal Study of Adolescent Health
(Add Health) database collected by Harris et al. (2003; Udry, 1997). This
is a school-based sample of 20,745 adolescents in Grades 7 through 12.
The sampling frame selected a random sample of 80 high schools. For each
school, a set of feeder schools was identified that included seventh and
eighth graders that sent their graduates to the high school. This resulted in
a pair of schools in each of 80 communities. Because some high schools
spanned Grades 7 to 12, they functioned as their own feeder school and the
pair was a single school. Adolescents in Grades 7 through 11 were
interviewed twice, with a 1-year interval between waves. Loss to follow-up
for unplanned reasons (e.g., refusals to be interviewed again, failure to
locate the respondent) was minimal (10%), with no significant biases.
Analyses were restricted to never married female adolescents in Grades 7
through 11 as reported at Wave 1 for a final sample size of 8,411. A
detailed description of the study is available at www.cpc.unc.edu/
addhealth.
Procedure
Interviews were administered in the respondents homes. All data were
recorded on laptop computers. For less sensitive sections, the interviewer
read the questions and entered the respondents answers. For more sensi-
tive sections, respondents listened to questions through earphones and
entered the answers directly on the computer. The topics covered in the
interviews were diverse, including health status, health utilization, nutri-
tion, educational aspirations, substance use, and criminal activities.
Measures
Perceived intelligence. Perceived intelligence was measured by asking
individuals to rate themselves on a scale in response to the following
question: Compared with other people your age, how intelligent are you?
The measure was scored on a 6-point rating scale, with higher scores
indicating higher levels of perceived intelligence: 1 moderately below
average, 2 slightly below average, 3 about average, 4 slightly
above average, 5 moderately above average, and 6 extremely above
average. A category called extremely below average was not included
because pilot research revealed that no one would mark this category.
Actual knowledge. Actual knowledge was measured in three domains:
knowledge about how to use condoms appropriately, knowledge about the
accurate use of the withdrawal method, and knowledge about the timing of
ovulation and when it is safe to have sex relative to ovulation. The most
common methods of birth control used by adolescents are condoms and
birth control pills, with many adolescents also relying on informal judg-
ments of ovulation timing. We selected the above three areas because we
felt that if an adolescent lacked knowledge about accurate use in these three
domains, the chances of an unintended pregnancy would be heightened. A
nine-item truefalse knowledge test was administered. The items were as
follows: When a woman has sexual intercourse, almost all sperm die
inside her body after about 6 hr; when using a condom, the man should
pull out of the woman right after he has ejaculated; natural skin (lamb
skin) condoms provide better protection against the AIDS virus than latex
condoms; when putting on a condom, it is important to have it fit tightly,
leaving no space at the tip; Vaseline can be used with condoms and they
will work just as well; the most likely time for a woman to get pregnant
is right before her period starts; even if a man pulls out before he
ejaculates (even if ejaculation occurs outside of the womans body), it is
still possible for the woman to become pregnant; as long as the condom
fits over the tip of the penis, it does not matter how far down it is unrolled;
and in general, a woman is most likely to get pregnant if she has sex
during her period, as compared to other times of the month. The mean
number of correct responses was the final score.
Perceived knowledge. Perceived knowledge was assessed with the
following three items: I am quite knowledgeable about the withdrawal
method of birth control; I am quite knowledgeable about the rhythm
method of birth control and when it is a safe time during the month for
a woman to have sex and not get pregnant; and I am quite knowledgeable
about how to use a condom correctly. Individuals responded on 5-point
164
JACCARD, DODGE, AND GUILAMO-RAMOS
agreedisagree scales (1 strongly disagree, 2 disagree, 3 neither,
4 agree, 5 strongly agree), where each of the items was separated by
filler items. Responses to the three items were averaged ( .78).
1
Self-esteem. Add Health used a short-form version of the Rosenberg
Self-Esteem Scale, which consisted of the following four items: I have a lot
of good qualities; I have a lot to be proud of; I like myself just the way I
am; I feel like I am doing everything just about right (Rosenberg, 1965).
Participants responded to each item on a 5-point agreedisagree scale (1
strongly disagree, 2 disagree, 3 neither, 4 agree, 5 strongly
agree). The four items had an average intercorrelation of .50 and yielded
an alpha coefficient of .80. The measure has concurrent validity in that it
was predictive of pregnancy outcomes as well as binge drinking tendencies
in the Add Health data sets. Pilot research revealed that the 4-item version
correlated .91 with the full 10-item Rosenberg scale (which includes the 4
items). A self-esteem score was based on the mean of the items such that
higher values indicated higher levels of self-esteem.
Academic aspirations. The academic aspirations of individuals were
assessed with the following two questions: On a 1 to 5 scale where 1 is
low and 5 is high, how much do you want to go to college? and On a 1
to 5 scale where 1 is low and 5 is high, how likely is it that you will go to
college? Responses to the two items were averaged ( .82).
IQ. IQ was measured with an abridged version of the Peabody Picture
Vocabulary TestRevised (PPVTR; Dunn & Dunn, 1981). The Add
Health version was computerized and involved the interviewer reading
aloud a word with the respondent selecting from four illustrations the one
that best reflected the meaning of the word. The scale was half the length
of the original Peabody Picture Vocabulary Test (PPVT), focusing on
every other item. The correlation between PPVT scores generated from a
standard administration of the original measure and the scores based on the
Add Health version is .96 (Halpern, Joyner, Udry, & Suchindran, 2000).
Scores on the scale were normed by age by using the traditional IQ metric
of a mean of 100 and a standard deviation of 15.
Conceptual definitions of intelligence are controversial. The PPVT has
a median correlation of .62 with the StanfordBinet Intelligence Scale and
a median correlation of .64 with the Wechsler Intelligence Scale for
Children. Our primary motivation in measuring IQ was to allow us to
evaluate the possibility that any correlation of perceived intelligence with
risk outcome is spurious because of the common influence of constructs
reflected by more general measures of IQ that have been shown to be
predictive of adolescent risk behavior. The PPVT has been shown to be
predictive of adolescent risk behavior in a number of domains and, hence,
fits the needs of the present research. The term IQ as used in this study,
however, is restricted to reflect the skills and abilities measured by the
PPVT.
Pregnancy outcome and sexual behavior. Three dichotomous behav-
ioral outcomes were measured at the second interview (approximately 1
year following the first interview): whether the respondent had engaged in
sexual intercourse since the time of the first interview, whether the respon-
dent used pregnancy protection at her most recent intercourse, and whether
the respondent had become pregnant since the time of the first interview.
The sexual intercourse measure was derived from responses to the follow-
ing question asked at both the first and second interviews: Have you ever
had sexual intercourse? When we say sexual intercourse, we mean when a
male inserts his penis into a females vagina. If the respondent reported
that he or she had never engaged in sexual intercourse at Wave 1 but had
engaged in sexual intercourse at Wave 2, then the respondent was scored
as having engaged in sexual intercourse since Wave 1. In addition, dates
provided in response to the question In what month and year did you have
sexual intercourse most recently? at Wave 2 were used to determine if
sexual intercourse had occurred since the last interview for adolescents
who were already sexually active as of Wave 1. Use of birth control was
assessed by asking individuals who had reported having sexual intercourse
to think of the last time they had done so and to indicate if they had used
a method to prevent a pregnancy and if so, to indicate what it was (from a
list of provided methods). Occurrence of a pregnancy between the first and
second interviews was derived from responses to the following item
measuring frequency of pregnancy: How many times have you been
pregnant? Responses were obtained to this item at both the first and
second interviews, and if the number of pregnancies increased, a pregnancy
was assumed to have occurred. Respondents also reported the date of their
most recent pregnancy, and this information was used to determine if a
pregnancy had occurred since Wave 1. If the reported date of a pregnancy
occurred between the time the adolescent was initially interviewed at Wave
1 and the time that she was interviewed at Wave 2, the adolescent also was
classified as having become pregnant between waves. Disparities between
the two forms of assessment were rare, and if either report suggested a
pregnancy, we classified the adolescent as having experienced a
pregnancy.
The primary outcome in our analyses was the occurrence of a pregnancy
between waves. We report subsidiary analyses with respect to the other two
indices of sexual risk taking.
Analytic Strategy
Although many of the conceptual issues were framed in a form that
suggests the use of traditional structural equation modeling, this approach
was not used because of the presence of a dichotomous endogenous
variable (the occurrence of a pregnancy). Traditional structural equation
modeling techniques cannot be applied in such cases. Instead, we used
limited information estimation strategies in the context of logistic regres-
sion (Bollen, 1996). The limited information estimation strategy relied on
directed logistic regressions that explicitly tested the predictions of the
model(s) for the causal paths in question.
Add Health used a stratified cluster sampling design in which schools
were sampled from the Quality of Education database. Sampling weights
were derived for both waves of the design by the project statisticians
(Tourangeau & Shin, 1999). These weights were used to calculate param-
eter estimates and standard errors in the statistical models. The community
from which the school was sampled served as the primary sampling unit.
Strata were defined in accord with the clustered sample design with a
minimum of two primary sampling units per stratum. Standard errors were
estimated by using the jack-knifing methods in the WesVar statistical
package (WesVar, 1998). The use of weighted versus unweighted data is
controversial among statisticians, with advocates in both camps (Lohr &
Liu, 1994; Winship & Radbill, 1994). Our analytic approach was to
analyze the data by using both weighted and unweighted analyses and to
focus only on effects that were robust across both forms of analysis. All of
the results were robust across the different forms of analysis. We report the
unweighted results.
The sample size in the analyses described below was approximately
8,411. Sample sizes varied slightly across analyses, depending on missing
data. Outlier analyses were performed for all analyses, as were checks for
model misspecification. Any analyses that included actual knowledge
about the accurate use of birth control typically had sample sizes of
approximately 5,339 because these questions were asked only of adoles-
cents who were at least 15 years of age.
1
It is possible that the order of assessment of knowledge and perceived
knowledge affects the measures of perceived knowledge. For example, if
individuals take a knowledge test prior to the assessment of perceived
knowledge, then this may alter their judgment about their knowledge
levels, depending on the difficulty of the test. Radecki and Jaccard (1995)
explored this possibility for a task involving birth control knowledge that
was similar to the present one and observed no such order effects. Also
important is whether there are floor or ceiling effects for either the actual
knowledge test or the perceived knowledge measures, as such base rate
problems may attenuate correlations between the constructs. We examined
the means and standard deviations of all measures for this possibility and
found no evidence for this.
165
METACOGNITION, RISK BEHAVIOR, AND RISK OUTCOMES
Results
Perceived Intelligence
Table 1 presents the frequency distribution of responses to the
perceived intelligence item. The distribution is skewed, with most
adolescents believing they are above average in intelligence. The
correlation between perceived intelligence and actual intelligence
was .28 (95% confidence interval [CI] 0.260.30, p .05),
suggesting a moderate correlation between the two constructs. The
mean intelligence scores for respondents at each point of the
perceived intelligence measure also appear in Table 1. In general,
there is a monotonic relationship between the perceived intelli-
gence ratings and the mean intelligence ratings, except at the
highest point on the scale, where there is a small decrease in mean
intelligence.
The bivariate relationship between the occurrence of a preg-
nancy and perceived intelligence was isolated by using logistic
regression in which the dichotomous outcome variable (reported a
pregnancy vs. did not report a pregnancy) was regressed onto the
perceived intelligence measure. The exponent of the logistic co-
efficient for perceived intelligence was 0.81 (95% CI 0.73
0.90, p .05), indicating that for every one unit that perceived
intelligence increased, the predicted odds of a pregnancy decreased
by a factor of 0.81. For example, when perceived intelligence was
at its lowest value, the predicted odds of a pregnancy was 0.08
(corresponding to a probability of .07), whereas when it was at its
highest value, the predicted odds of a pregnancy was only 0.03
(corresponding to a probability of .029). The relationship between
perceived intelligence and pregnancy occurrence was evaluated
with grade, ethnicity, maternal education, and family income in-
cluded as covariates. In all analyses reported hereafter, these
covariates are included in the logistic analyses unless otherwise
noted. Results tended to be the same whether or not the covariates
were included in the model.
To address whether perceived intelligence was related to the
occurrence of a pregnancy independent of IQ, we performed a
logistic regression analysis to predict pregnancy outcome from the
perceived intelligence scores and the PPVT scores. Model diag-
nostics suggested a curvilinear effect for PPVT in the form of an
inverted U shape, and the addition of a squared PPVT score to the
initial equation yielded a statistically significant logistic coeffi-
cient. In general, the predicted odds of a pregnancy tended to be
lower at the low and high ends of the PPVT and tended to peak at
a PPVT score of approximately 90. For this reason, all analyses
that include IQ as a covariate used both the PPVT scores and the
squared PPVT scores as predictors. For the equation regressing
pregnancy outcome onto perceived intelligence, intelligence, and
the demographic covariates, the logistic coefficient for perceived
intelligence was statistically significant, with the exponent of the
coefficient equaling 0.84 (95% CI 0.750.95, p .05). This
suggests that perceived intelligence is related to the occurrence of
a pregnancy independent of its association with actual intelligence
(as measured by the PPVT), with higher levels of perceived
intelligence leading to lower odds of a pregnancy. The IQ score
also was a statistically significant predictor of pregnancy occur-
rence independent of perceived intelligence. These data are incon-
sistent with the spurious effect model and the mediator model in
Figure 1 and are consistent with the independent effect model.
It is possible that perceived intelligence merely reflects the
dynamics of self-esteem (with higher levels of perceived intelli-
gence being associated with higher levels of self-esteem). To
evaluate the potential mediating role of self-esteem in the inde-
pendent effects model, we included the measure of self-esteem in
the logistic regression that used perceived IQ, actual intelligence,
and the covariates as predictors. If the influence of perceived
intelligence derives from its association with self-esteem, then the
logistic coefficient for perceived intelligence should change to
nonsignificance or be trivial in value. The exponent of the coeffi-
cient for perceived IQ in this equation was 0.86 (95% CI
0.760.97, p .05), and it maintained its statistical significance.
This suggests that the bases of the predictive power of perceived
intelligence are not necessarily captured by self-esteem. Parenthet-
ically, self-esteem also made an independent contribution to pre-
dicting the log odds of a pregnancy, yielding a coefficient with an
exponent of 0.83 (95% CI 0.690.99, p .05). Higher levels
of self-esteem were associated with lower levels of pregnancy.
A second analysis evaluated whether the effects of perceived
intelligence could be attributed to its relationship to academic
aspirations. The most likely model is one involving mediation such
that those who believe themselves to be more intelligent set higher
academic aspirations as a result of their supposed higher intellect.
These higher aspirations, in turn, impact the occurrence of a
pregnancy. When academic aspirations were substituted for self-
esteem in the logistic analyses, the exponent of the coefficient for
perceived intelligence was 0.87 (95% CI 0.780.98, p .05).
Perceived intelligence maintained its independent effect on the
occurrence of a pregnancy, suggesting that academic aspirations
were not the source of its effects. Parenthetically, academic aspi-
rations were predictive of pregnancy occurrence independent of
perceived intelligence and intelligence (exponent of logistic coef-
ficient 0.78, 95% CI 0.700.87, p .05), such that students
with higher academic aspirations had a lower probability of a
pregnancy.
Taken together, these analyses suggest that the effects of per-
ceived intelligence are not simply attributable to confounds with
self-esteem or academic aspirations. The data are consistent with
effects of perceived intelligence independent of these mechanisms.
Perceived Knowledge
The correlation between perceived and actual knowledge was
.10 (95% CI 0.070.13, p .05). These data suggest a statis-
tically significant but weak association between perceived knowl-
edge and actual knowledge and are consistent with the results of
Radecki and Jaccard (1995). To test if perceived knowledge was
associated with the occurrence of a pregnancy independent of
Table 1
Perceived Intelligence Frequency Distribution and Mean
Intelligence Scores
Category Frequency % Mean PPVTR
Moderately below average 100 1.2 83.7
Slightly below average 376 4.5 91.7
About average 3,423 40.7 95.0
Slightly above average 1,773 21.2 101.8
Moderately above average 2,160 25.7 104.6
Extremely above average 551 6.6 100.4
Note. PPVTR Peabody Picture Vocabulary TestRevised.
166
JACCARD, DODGE, AND GUILAMO-RAMOS
actual knowledge, we performed a logistic regression that re-
gressed the occurrence of a pregnancy onto the covariates, per-
ceived knowledge, and actual knowledge. The exponent of the
logistic coefficient was 1.53 (95% CI 1.281.81, p .05),
suggesting that higher levels of perceived knowledge were asso-
ciated with a higher probability of a pregnancy during the ensuing
year. For every one unit that perceived knowledge changed (on the
five-category scale on which it was measured), the predicted odds
of a pregnancy increased by a multiplicative factor of 1.53, holding
actual knowledge constant. When perceived knowledge was at its
highest level, the predicted odds of a pregnancy was over seven
and a half times higher than when perceived knowledge was at its
lowest value. The exponent of the coefficient for actual knowledge
was 2.70 (95% CI 1.385.31, p .05), indicating that higher
levels of actual knowledge were associated with higher probabil-
ities of a pregnancy. This latter result was unexpected, as we had
hypothesized that those with higher levels of knowledge about the
accurate use of birth control would be less likely to experience a
pregnancy.
To test if the impact of perceived knowledge on pregnancy
occurrence was moderated by actual knowledge, we reestimated
the logistic regression equation but included a product term be-
tween perceived knowledge and actual knowledge. The product
term was not statistically significant and was trivial in magnitude
(exponent of logistic coefficient 1.78, 95% CI 0.833.84).
The results of these analyses are inconsistent with the model that
holds that the impact of perceived knowledge is moderated by the
effects of actual knowledge. Instead, higher levels of perceived
knowledge are associated with a higher probability of pregnancy
irrespective of the levels of actual knowledge. The model that
predicted this outcome posited that the effect was due to the fact
that those who thought they were more knowledgeable about the
accurate use of birth control would be more likely to engage in sex.
To test this possibility, we performed a logistic regression analysis
that regressed whether the individual had engaged in sex between
Wave 1 and Wave 2 onto the covariates, perceived knowledge (as
measured at Wave 1), and actual knowledge (as measured at Wave
1). The exponent of the logistic coefficient for perceived knowl-
edge was 1.66 (95% CI 1.541.80, p .05), indicating that
those with higher levels of perceived knowledge about the accurate
use of birth control had a higher probability of engaging in sexual
intercourse. The exponent of the logistic coefficient for actual
knowledge was 4.03 (95% CI 2.935.54, p .05), indicating
that more knowledge about the accurate use of birth control at
Wave 1 was associated with a higher probability of sexual inter-
course during the ensuing year.
Although the above results are consistent with the proposition
that higher levels of perceived knowledge about birth control
dispose the individual toward engaging in sexual intercourse, it is
possible that the causal influence is in the reverse direction, with
individuals who engage in more sexual activity becoming more
confident of their knowledge about the accurate use of birth
control by virtue of their greater experience with sex. The per-
ceived knowledge measure was obtained at Wave 1, whereas the
sexual behavior measure was obtained 1 year later, thereby ques-
tioning this interpretation. In addition, we tested if the effects of
perceived knowledge on sexual activity persisted if virgin status at
Wave 1 was introduced as a covariate into the equation (thereby
controlling for initial levels of sexual activity), and this was indeed
the case. Finally, perceived knowledge at Wave 1 was predictive
of sexual activity between the two waves even when perceived
knowledge at Wave 2 was included as a covariate in the equation
(exponent of the logistic coefficient for Wave 1 perceived knowl-
edge 1.26, 95% CI 1.151.37, p .05). Taken together, these
results question (but do not rule out definitively) the interpretation
that the causal direction is strictly from sexual activity to perceived
knowledge.
Another possible source of spuriousness is that adolescents
acquire information about birth control when they are about to
become sexually active and that the information acquisition activ-
ities that they engage in during this time increase their perceived
knowledge about birth control. Higher levels of perceived knowl-
edge do not bias the individual to engage in sex. Rather, the higher
levels of perceived knowledge reflect the fact that the individual is
preparing for sex and has participated in some information-
acquisition activities. One way to address this issue is to include
covariates in the analysis that serve as indicators of whether an
individual at Wave 1 is preparing for sex. If the effects of per-
ceived knowledge on sexual activity are merely the result of
preparing for sex, then the logistic coefficient for perceived knowl-
edge should vanish when these covariates are included. We added
three such indicators to the logistic regression (in addition to the
standard covariates, perceived knowledge, and actual knowledge):
(a) whether the adolescent was currently involved in a romantic
relationship (on the assumption that those who are involved in a
relationship are more likely to be preparing for sex than those who
are not), (b) an index of physical development (on the assumption
that those who are more physically mature are more likely to be
preparing for sex than those who are less physically mature), and
(c) whether the adolescent was a virgin at Wave 1 (on the assump-
tion that nonvirgins would be more likely to be preparing for future
sex). The logistic coefficient for perceived knowledge remained
statistically significant in this analysis (exponent of logistic coef-
ficient 1.22, 95% CI 1.121.34, p .05).
In sum, the analyses suggest that those with higher levels of
perceived knowledge about the accurate use of birth control are at
greater risk for a pregnancy independent of their actual knowledge
about the accurate use of birth control and that the source of this
may be their tendency to greater exposure to sexual situations.
Perceived Intelligence and Perceived Knowledge
To explore the relationship between perceived intelligence and
perceived knowledge, we calculated the correlation between the
two constructs. The correlation was .05 (95% CI 0.07 to
0.03, ns). This correlation suggests a trivial relationship between
the constructs and is counter to both the halo-effects and defen-
siveness models. It is not surprising (in light of these correlations)
that perceived knowledge was predictive of the occurrence of a
pregnancy even when perceived intelligence was included as a
covariate in the logistic regression equation (exponent of logistic
coefficient 1.52, 95% CI 1.281.81, p .05), and this was
also true when perceived intelligence, actual intelligence, self-
esteem, academic aspirations, academic performance, and actual
knowledge were included as covariates (exponent of logistic co-
efficient 1.44, 95% CI 1.201.73, p .05).
Mediators of the Occurrence of a Pregnancy
The occurrence of a pregnancy between waves is influenced, in
part, by two behavioral mediators: the amount of sexual activity
167
METACOGNITION, RISK BEHAVIOR, AND RISK OUTCOMES
that an adolescent engages in and the extent to which pregnancy
protection is used during sexual intercourse. The Add Health data
had limited measures of these constructs, such that we could only
define (a) whether an individual had engaged in sex between
waves and (b) whether the individual had used some form of
pregnancy protection at her most recent intercourse. The construct
of perceived intelligence was related to both of these outcomes, as
reflected in two separate logistic regressions. In general, higher
perceived intelligence was associated with lower levels of sexual
activity (exponent of coefficient 0.88, 95% CI 0.840.92,
p .05) and higher levels of birth control use (exponent of
coefficient 1.16, 95% CI 1.071.26, p .05). Perceived
knowledge was only statistically significantly related to sexual
activity, such that higher perceived knowledge was associated with
higher levels of sexual activity (exponent of coefficient 1.68,
95% CI 1.591.79, p .05). These results were robust when
demographic covariates were included in the model as well as
when perceived intelligence, perceived knowledge, actual knowl-
edge, and actual IQ all were included in the equations.
Discussion
Perceptions of ones knowledge as well as more abstract per-
ceptions of ones intelligence represent central constructs in meta-
cognitive theory. The present study was one of the first empirical
demonstrations of a link between these constructs and risk behav-
ior and risk outcomes. The results suggest that both constructs are
independently tied to risk behavior and risk outcomes and exert
effects on such behavior over and above actual IQ and actual
knowledge.
With respect to perceived intelligence, we found that individuals
tended to perceive themselves as above average in intellect, at least
as reflected by labels on our rating scales. Perceived intelligence
served a protective function such that higher levels of perceived
intelligence were associated with lower probabilities of adverse
risk outcomes. The effects of perceived intelligence could not be
accounted for by IQ, as measured by the PPVTR, nor could the
effects be accounted for by self-esteem or academic aspirations.
Perceived intelligence seems to contribute explanatory power over
and above these more traditional constructs.
Whereas higher levels of perceived intellect were protective
when considered at the abstract level, just the opposite was found
for perceived knowledge at the specific level. As perceived knowl-
edge about strategies for avoiding the negative consequences of a
risk behavior increased (holding actual knowledge constant), the
likelihood of experiencing those consequences also increased.
Three different models relating perceived knowledge to risk out-
comes were evaluated. The most viable model seemed to be one
that argued that higher levels of knowledge about strategies to
avoid negative outcomes result in increased performance of risk
behaviors, perhaps because the threat of the negative consequences
has been lessened. This increased exposure to risk, in turn, raises
the probability of experiencing an adverse outcome.
The overall picture that emerges is one of diametrically opposed
processes operating for metacognition and risk behavior that de-
pend on the level of abstractness of the metacognition. These
processes are independent of one another, as reflected by the weak
and inconsistent correlation between perceived intelligence on the
one hand and perceived knowledge about the strategies for avoid-
ing risk behavior on the other, as well as by the fact that perceived
intelligence failed to mediate any of the effects of perceived
knowledge on risk outcomes and vice versa. At the abstract level,
metacognitive constructs such as perceived intelligence may im-
pact broad-based lifestyles (e.g., working hard in school) that serve
to push the individual toward constructive activities and away
from counterproductive risk behaviors. At the specific level, per-
ceptions that one has the requisite knowledge base to avoid neg-
ative consequences of risk behavior may encourage the individual
to engage in such behaviors, thereby raising the risk to the indi-
vidual. Future research needs to further explore this potentially
interesting dynamic of opposing risk and protective functions.
The results of this study have applied implications. For example,
an emerging strategy for the prevention of risk behavior in ado-
lescents is one based on increasing communication between par-
ents and children about problem behaviors (Jaccard, Dittus, &
Litardo, 1999). Studies of reasons parents provide for not engaging
in conversations with their adolescents about a given risk behavior
suggest that a common reason is that their adolescents profess to
already know what they need to know about the behavior (e.g.,
drugs, sex, alcohol; see Jaccard & Dittus, 1991). The present data
suggest that rather than be deterred by such statements, parents
should be all that more concerned, because adolescents who claim
higher levels of perceived knowledge actually may be at greater
risk. Another potential ramification focuses on the presentation of
educational information about risk behavior and ways of avoiding
risk outcomes. As adolescents are exposed to such information,
their perceptions of how knowledgeable they are may increase.
The effect of such information provision may actually have ad-
verse effects if the information is not directly acted upon by the
adolescent because the increased levels of perceived knowledge
about how to avoid the consequences of risk behavior may dispose
the individual to engage in more risk behavior out of the belief that
she or he can avoid the adverse consequences.
Several ancillary findings were observed in the present research
that, though not the focus of the study, are worthy of future
investigation. The first result was the observation of a curvilinear
relationship between IQ as measured by the PPVTR and the
occurrence of a pregnancy between Wave 1 and Wave 2. The
probability of a pregnancy tended to be lowest for individuals of
low and high intelligence and tended to peak for individuals who
were near or just below average intelligence. Using the Add Health
database, Halpern et al. (2000) found that intelligence was curvi-
linearly related to sexual behavior in a fashion similar to this study.
Our results extend this finding to pregnancy occurrence. The
mechanisms that can account for this interesting relationship need
to be further explored. A second result of interest was the finding
that increasing levels of knowledge about the accurate use of birth
control were associated with an increased probability of both
sexual behavior and a pregnancy between Wave 1 and Wave 2.
This finding has potential policy implications as it suggests a link
between the acquisition of information about birth control and
subsequent sexual activity. This is a complex issue, and the anal-
yses reported here are insufficient to gain perspectives on the many
possible alternative explanations of this result. Future research
should explore this finding in greater depth.
The present analysis, though provocative, has limitations that
must be borne in mind. The study used only a single risk behavior,
and it is unclear if the socialpsychological dynamics will replicate
with other risk behaviors. We relied on a school-based sample that
does not, strictly speaking, permit generalizations beyond such
168
JACCARD, DODGE, AND GUILAMO-RAMOS
populations. It is possible that variation in the knowledge test was
due, in part, to a failure of some of the adolescents to understand
the questions rather than to the lack of knowledge per se. The Add
Health questionnaire was pilot tested for comprehension, and the
knowledge questions were only asked of adolescents who were
older than 14 or who were sexually active, thus lessening this
possibility.
2
The research also relied on self-report measures of
pregnancy, which also represents a cause for caution because such
reports may contain some error. Questions about sex and preg-
nancy were posed to adolescents through headphones on a laptop
computer, and the adolescent entered her response so that no one
could see it. The respondent also knew that her name would never
be associated with the data in any way. Adolescents were given
instructional sets that emphasized the importance of honest re-
sponding. Adolescents had the option of skipping questions they
felt uncomfortable answering. We correlated the self-report of a
pregnancy with a measure of social-desirability response tenden-
cies, and the correlation was trivial and not significant. Although
we doubt that there is sufficient error to undermine the conclusions
of the present study, one still must be cautious. The design of the
study was correlational in nature, and many of the constructs were
represented by a single measure, introducing potential bias in
parameter estimates because of measurement error. If a construct
is not adequately represented by a measure, then that construct
may not be fully controlled for in the statistical analyses. Despite
these caveats, the results are suggestive and set the stage for further
research on metacognition and risk behavior.
2
The correlation between the knowledge scores and scores on the IQ test
was .27, suggesting that adolescents with higher levels of receptive vocab-
ulary were more likely to obtain higher knowledge scores. One might
expect on logical grounds that adolescents with higher IQs should indeed
be more knowledgeable about pregnancy prevention than adolescents with
lower IQs, but we cannot rule out conclusively that some of this correlation
reflects the possibility that adolescents with lower receptive vocabulary
were less able to understand some of the knowledge items.
References
Anderson, N. H. (1981). Foundations of information integration theory.
New York: Academic Press.
Bailey, R. C. (1971). Self-concept differences in low and high achieving
students. Journal of Clinical Psychology, 27, 188191.
Bailey, R. C., & Mettetal, G. W. (1977). Sex differences in the congruency
of perceived intelligence. Journal of Genetic Psychology, 131, 2936.
Bandura, A. (1986). Social foundations of thought and action: A social
cognitive theory. Englewood Cliffs, NJ: Prentice Hall.
Bandura, A. (1989). Human agency on social cognitive theory. American
Psychologist, 44, 11751184.
Bollen, K. (1996). A limited information estimator for LISREL models
with or without heteroscedastic errors. In G. Marcoulides & R. Schu-
macker (Eds.), Advanced structural equation modeling: Issues and tech-
niques (pp. 227242). Mahwah, NJ: Erlbaum.
Cliquet, R. L., & Balcaen, J. (1983). Intelligence, family planning and
family formation. In R. Cliquet, G. Dooghe, D. Van de Kaa, & H. Moors
(Eds.), Population and family in the low countries III (Vol. 10, pp.
2770). Voorsburg: Netherlands Interuniversity Demographic Institute.
Dunn, L. M., & Dunn, L. (1981). Peabody Picture Vocabulary Test
Revised: Manual for Forms L and M. Circle Pines, MN: American
Guidance Service.
Epstein, W., Glenberg, A. M., & Bradley, M. M. (1984). Coactivation and
comprehension: Contribution of text variables to the illusion of knowing.
Memory & Cognition, 12, 355360.
Gabriel, M. T., Critelli, J. W., & Ee, J. (1994). Narcissistic illusions in
self-evaluations of intelligence and attractiveness. Journal of Personal-
ity, 62, 143155.
Gentner, D., & Collins, A. (1981). Studies of inference from lack of
knowledge. Memory & Cognition, 9, 434443.
Glenberg, A. M., Wilkinson, A. C., & Epstein, W. (1982). The illusion of
knowing: Failure in the self-assessment of comprehension. Memory &
Cognition, 10, 597602.
Glucksberg, S., & McCloskey, M. (1981). Decisions about ignorance:
Knowing that you dont know. Journal of Experimental Psychology:
Human Learning and Memory, 7, 311325.
Griffin, H. W., Botvin, G., Doyle, M., Diaz, T., & Epstein, J. (1999). A
six-year follow-up study of determinants of heavy cigarette smoking
among high school seniors. Journal of Behavioral Medicine, 22, 271
284.
Halpern, C. T., Joyner, K., Udry, J. R., & Suchindran, C. (2000). Smart
teens dont have sex (or kiss much either). Journal of Adolescent Health,
26, 213225.
Harris, K. M., Florey, F., Tabor, J., Bearman, P. S., Jones, J., & Udry, J. R.
(2003). The National Longitudinal Study of Adolescent Health: Re-
search design. Retrieved October 28, 2004, from http://www
.cpc.unc.edu/projects/addhealth/design
Jaccard, J., & Dittus, P. (1991). Parentteenager communication: Toward
the prevention of unintended pregnancies. New York: Springer-Verlag.
Jaccard, J., Dittus, P., & Litardo, H. (1999). Parentadolescent communi-
cation about sex and birth control: Implications for parent-based inter-
ventions to reduce unintended adolescent pregnancy. In W. Miller & L.
Severy (Eds.), Advances in population research: Psychosocial perspec-
tives (pp. 220246). London: Kingsley.
Jang, S., & Thornberry, T. (1998). Self-esteem, delinquent peers, and
delinquency: A test of the self-enhancement thesis. American Sociolog-
ical Review, 63, 586598.
Jessor, R., Costa, F., Jessor, S. L., & Donovan, J. (1983). The time of first
intercourse: A prospective study. Journal of Personality and Social
Psychology, 44, 608619.
Jost, J. T., Kruglanski, A., & Nelson, T. (1999). Social metacognition: An
expansionist review. Personality and Social Psychology Review, 2,
137154.
Kasen, S., Cohen, P., & Brook, J. (1997). Adolescent school experiences
and dropout, adolescent pregnancy, and young adult deviant behavior.
Journal of Adolescent Research, 13, 4972.
Keren, G. (1991). Calibration and probability judgments: Conceptual and
methodological issues. Acta Psychologica, 77, 217273.
Kolers, P. A., & Palef, S. R. (1976). Knowing not. Memory & Cognition,
4, 553558.
Kruger, J., & Dunning, D. (1999). Unskilled and unaware of it: How
difficulties in recognizing ones own incompetence lead to inflated
self-assessments. Journal of Personality and Social Psychology, 77,
11211134.
Lent, R. W., Brown, S. D., & Larkin, K. C. (1984). Relation of self-
efficacy expectations to academic achievement and persistence. Journal
of Counseling Psychology, 31, 356362.
Lichenstein, S., & Fischoff, B. (1977). Do those who know more also know
more about how much they know? The calibration of probability judg-
ments. Organizational Behavior and Human Performance, 20, 159183.
Lohr, S. L., & Liu, J. (1994). A comparison of weighted and unweighted
analyses in the National Crime Victimization Survey. Journal of Quan-
titative Criminology, 10, 343360.
Metcalfe, J., & Shimamura, A. P. (1994). Metacognition: Knowing about
knowing. Cambridge, MA: MIT Press.
Moffit, T. E., Gabrielli, W. F., Mednick, S. A., & Schulsinger, F. (1981).
169
METACOGNITION, RISK BEHAVIOR, AND RISK OUTCOMES
Socioeconomic status, IQ, and delinquency. Journal of Abnormal Psy-
chology, 90, 152159.
Mott, F. L. (1983, November). Early fertility behavior among American
youth: Evidence from the 1982 National Longitudinal Surveys of Labor
Force Behavior of Youth. Paper presented at the American Public Health
Meetings, Dallas, TX.
Nelson, T. (1992). Metacognition: Core readings. Needham Heights, MA:
Allyn & Bacon.
Nelson, T. O., Gerler, D., & Narens, L. (1984). Accuracy of feeling-of-
knowing judgments for predicting perceptual identification and relearn-
ing. Journal of Experimental Psychology: General, 113, 282300.
Nelson, T. O., Kruglanski, A. W., & Jost, J. T. (1998). Knowing thyself
and others: Progress in metacognitive social psychology. In. V. Yzerbyt,
G. Lories, & B. Dardenne (Eds.), Metacognition: Cognitive and social
dimensions (pp. 6989). London: Sage.
Oetting, E. R., Deffenbacher, J. L., & Donnermeyer, J. F. (1998). Primary
socialization theory: The role played by personal traits in the etiology of
drug use and deviance: II. Substance Use & Misuse, 33, 13371366.
Parsons, J. E. (1983). Expectancies, values, and academic behaviors. In
J. T. Spence (Ed.), Achievement and achievement motives (pp. 75146).
San Francisco: Freeman.
Pederson, L., Koval, J., McGrady, G., & Tyas, S. (1998). The degree and
type of relationship between psychosocial variables and smoking status
for students in Grade 8: Is there a doseresponse relationship? Preven-
tive Medicine, 27, 337347.
Quadrel, M. J., Fischoff, B., & Davis, W. (1993). Adolescent (in)vulner-
ability. American Psychologist, 48, 102116.
Radecki, C. M., & Jaccard, J. (1995). Perceptions of knowledge, actual
knowledge, and information search behavior. Journal of Experimental
Social Psychology, 31, 107138.
Raine, T. R., Jenkins, R., Aarons, S., Woodward, K., & Fairfax, J. (1999).
Sociodemographic correlates of virginity in seventh-grade Black and
Latino students. Journal of Adolescent Health, 24, 304312.
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton,
NJ: Princeton University Press.
Ruble, D. N., Boggiano, A. K., Feldman, N. S., & Loebl, J. H. (1980).
Developmental analysis of the role of social comparison in self-
evaluation. Developmental Psychology, 16, 105115.
Ruffman, T. K., & Olson, D. R. (1989). Childrens ascriptions of knowl-
edge to others. Developmental Psychology, 25, 601606.
Schacter, D. L. (1983). Feeling of knowing in episodic memory. Journal of
Experimental Psychology: Learning, Memory, and Cognition, 9, 3954.
Stipek, D., & MacIver, D. (1989). Developmental change in childrens assess-
ment of intellectual competence. Child Development, 60, 521538.
Strack, F., & Forester, J. (1999). Self-reflection and recognition: The role
of metacognitive knowledge in the attribution of recollective experience.
Personality and Social Psychology Review, 2, 111123.
Tourangeau, R., & Shin, H. C. (1999). The National Longitudinal Study of
Adolescent Health: Grand sample weights. Chapel Hill: Carolina Pop-
ulation Center, University of North Carolina.
Udry, J. R. (1997). A research design for studying romantic partners. In J.
Bancroft (Ed.), Researching sexual behavior: Methodological issues
(pp. 237250). Bloomington: Indiana University Press.
Weiner, B. (1994). Ability versus effort revisited: The moral determinants
of achievement evaluation and achievement as a moral system. Educa-
tional Psychologist, 29, 163172.
Weiner, B., Russell, D., & Lerman, D. (1979). The cognitionemotion
process in achievement-related contexts. Journal of Personality and
Social Psychology, 37, 12111220.
WesVar. (1998). WesVar complex samples 3.0: Users guide. Chicago:
SPSS.
Wimmer, H., Hogrefe, J., & Perner, J. (1988). Childrens understanding of
informational access as a source of knowledge. Child Development, 59,
386396.
Winship, C., & Radbill, L. (1994). Sampling weights and regression
analysis. Sociological Methods and Research, 23, 230257.
Wood, R., & Bandura, A. (1989). Impact of conceptions of ability on
self-regulatory mechanisms and complex decision making. Journal of
Personality and Social Psychology, 56, 407415.
Yzerbyt, G., & Lories, G. (1999). Metacognition: Cognitive and social
dimensions. Thousand Oaks, CA: Sage.
170
JACCARD, DODGE, AND GUILAMO-RAMOS
Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Module On Organization and ManagementDocumento10 pagineModule On Organization and ManagementEmarilyn Bayot76% (21)
- RPH English KSSM Form 1 - Week 1Documento3 pagineRPH English KSSM Form 1 - Week 1Cikgu Mie100% (11)
- Chestionar Perfectionism in The Self and Social ContextsDocumento15 pagineChestionar Perfectionism in The Self and Social Contexts119568Nessuna valutazione finora
- Retrieval Fluency Contribute To The UNDERCONFIDENCEDocumento9 pagineRetrieval Fluency Contribute To The UNDERCONFIDENCE119568Nessuna valutazione finora
- Met A CognitionDocumento4 pagineMet A Cognition119568Nessuna valutazione finora
- Memorie Strategica La CopiiDocumento8 pagineMemorie Strategica La Copii119568Nessuna valutazione finora
- Anexa 6: Case Processing SummaryDocumento1 paginaAnexa 6: Case Processing Summary119568Nessuna valutazione finora
- ANEXA 5 - PearsonDocumento1 paginaANEXA 5 - Pearson119568Nessuna valutazione finora
- My DocumentsDocumento25 pagineMy DocumentsAbdurazak ArarsaNessuna valutazione finora
- Methods of Teaching English As A Foreign Language Task 2Documento7 pagineMethods of Teaching English As A Foreign Language Task 2IVONNE GARCIANessuna valutazione finora
- 77-1557305671121-Unit 6 Managing A Successful Computing Research Project 2019Documento14 pagine77-1557305671121-Unit 6 Managing A Successful Computing Research Project 2019Kevin JeromNessuna valutazione finora
- Report On Events On Education DayDocumento2 pagineReport On Events On Education Dayrajeevv_6Nessuna valutazione finora
- The History of Claredita FallsDocumento6 pagineThe History of Claredita FallsJann Romene Decena100% (1)
- DLL G6 Q1 Week 2 All SubjectsDocumento45 pagineDLL G6 Q1 Week 2 All SubjectsArenas JenNessuna valutazione finora
- Guidelines For Teaching Pronunciation: February 2019Documento6 pagineGuidelines For Teaching Pronunciation: February 2019رحمة الجنيديNessuna valutazione finora
- Masa Depan Profesi Akuntansi Dalam Revolusi Industri 4.0: Analisis Meta-Sintesis AbstrakDocumento15 pagineMasa Depan Profesi Akuntansi Dalam Revolusi Industri 4.0: Analisis Meta-Sintesis AbstrakHoàng Hải QuyênNessuna valutazione finora
- Operant ConditioningDocumento14 pagineOperant Conditioningniks2409Nessuna valutazione finora
- Lessonplan 1Documento5 pagineLessonplan 1api-272727134Nessuna valutazione finora
- MYP Mid Assessment (Writing) PDFDocumento4 pagineMYP Mid Assessment (Writing) PDFtaliaNessuna valutazione finora
- Avatar and IepDocumento7 pagineAvatar and Iepapi-249199136Nessuna valutazione finora
- English Language Research For Speaking As A Foreing LangDocumento31 pagineEnglish Language Research For Speaking As A Foreing LangSARALA A/P S.K.SUBRAMANYAM MoeNessuna valutazione finora
- GCSE Sciences:: What Are You Being Asked To Do in The Exams?Documento1 paginaGCSE Sciences:: What Are You Being Asked To Do in The Exams?Eseel AlsammarraieNessuna valutazione finora
- Micro TeachingDocumento32 pagineMicro Teachingmhel20010Nessuna valutazione finora
- Support Vector Machines: Trends & ControversiesDocumento11 pagineSupport Vector Machines: Trends & ControversiesEZ112Nessuna valutazione finora
- ORGB 4 4th Edition Nelson Solutions Manual 1Documento43 pagineORGB 4 4th Edition Nelson Solutions Manual 1shirley100% (44)
- Teacher's Book 3AMDocumento158 pagineTeacher's Book 3AMtitebin81% (37)
- Morphed Animal Rubric 2015Documento1 paginaMorphed Animal Rubric 2015api-325718341Nessuna valutazione finora
- Etd9534 ACant PDFDocumento228 pagineEtd9534 ACant PDFDiana PopNessuna valutazione finora
- Learning Delivery Modalities Output Lac Group 4Documento20 pagineLearning Delivery Modalities Output Lac Group 4Rafaela VillanuevaNessuna valutazione finora
- Self-Presentation For Utm, Skudai, JohorDocumento12 pagineSelf-Presentation For Utm, Skudai, JohorAmy RoslanNessuna valutazione finora
- Kapil: Curriculam VitaeDocumento2 pagineKapil: Curriculam VitaeDeepak SinghalNessuna valutazione finora
- Purposive CommunicationDocumento1 paginaPurposive CommunicationArt Lloyd DatahanNessuna valutazione finora
- Introduce Your Friend To The ClassDocumento2 pagineIntroduce Your Friend To The Classgustavo jaramilloNessuna valutazione finora
- Lester Choi'sDocumento1 paginaLester Choi'sca5lester12Nessuna valutazione finora
- Research Methods in Cognitive PsychologyDocumento3 pagineResearch Methods in Cognitive Psychologyi am PerfectNessuna valutazione finora
- Unit Plan Number PatternsDocumento14 pagineUnit Plan Number Patternsapi-525241634Nessuna valutazione finora