Potrebbero piacerti anche
- Nursing care process in patients with chronic obstructive pulmonary diseaseDa EverandNursing care process in patients with chronic obstructive pulmonary diseaseNessuna valutazione finora
- ICU Scoring Systems A Complete Guide - 2020 EditionDa EverandICU Scoring Systems A Complete Guide - 2020 EditionNessuna valutazione finora
- DOCU - MedA Charting GuidelinesDocumento3 pagineDOCU - MedA Charting GuidelinesTee Wood50% (2)
- Philosophy of NursingDocumento8 paginePhilosophy of Nursingapi-430575435Nessuna valutazione finora
- vSim CLINICAL REPLACEMENT PACKETDocumento14 paginevSim CLINICAL REPLACEMENT PACKETBhargav DaveNessuna valutazione finora
- The New Rapid ResponderDocumento3 pagineThe New Rapid RespondersarahNessuna valutazione finora
- Family Medicine M3 Clerkship: Hypertensive Disorders GuideDocumento35 pagineFamily Medicine M3 Clerkship: Hypertensive Disorders GuideJT ThomasNessuna valutazione finora
- Physical Assessment ChecklistDocumento3 paginePhysical Assessment ChecklistIsang ButaNessuna valutazione finora
- Evolve Key Points and Questions For Test 2 Maternal Child CareDocumento104 pagineEvolve Key Points and Questions For Test 2 Maternal Child CareHeather100% (2)
- TXTDocumento356 pagineTXTJec AmracNessuna valutazione finora
- Heart and Neck AssessmentDocumento3 pagineHeart and Neck AssessmentKiara Ash BeethovenNessuna valutazione finora
- CH 31 - Assessment and Management of Patients With Vascular Disorders and Problems of PeripheralDocumento16 pagineCH 31 - Assessment and Management of Patients With Vascular Disorders and Problems of PeripheralPye Antwan DelvaNessuna valutazione finora
- Physical Examination Techniques and ManueversDocumento160 paginePhysical Examination Techniques and ManueversMa-anJaneDiamosNessuna valutazione finora
- Clinical Paperwork For StudentsDocumento16 pagineClinical Paperwork For StudentsRyanNessuna valutazione finora
- Personal Philosophy of NursingDocumento7 paginePersonal Philosophy of Nursingapi-401205232Nessuna valutazione finora
- Outcomes of Ebp Process 2017Documento3 pagineOutcomes of Ebp Process 2017api-272725467100% (1)
- 2melnyk Ebp The Seven StepsDocumento3 pagine2melnyk Ebp The Seven Stepsapi-272725467100% (1)
- Ch35 CardiovascularDocumento11 pagineCh35 CardiovascularJessie Jennings100% (3)
- Head, Mouth, Nose, Throat, Neck and Regional Lymph Nodes: Kristin Clephane, MSN, RN, CPNDocumento44 pagineHead, Mouth, Nose, Throat, Neck and Regional Lymph Nodes: Kristin Clephane, MSN, RN, CPNMike100% (1)
- Running Head: NURSING STANDARDS 1Documento20 pagineRunning Head: NURSING STANDARDS 1api-253509573Nessuna valutazione finora
- Emergency Guidelines for Medical EmergenciesDocumento72 pagineEmergency Guidelines for Medical EmergenciesRumana Ali100% (2)
- Nursing Diagnosis TemplateDocumento6 pagineNursing Diagnosis Templatesdk6972Nessuna valutazione finora
- Cad PPTDocumento81 pagineCad PPTvaishnaviNessuna valutazione finora
- Week 2 InitialDocumento2 pagineWeek 2 InitialSara NielsenNessuna valutazione finora
- Chapter 1. Issues and Trends in Pediatric Nursing: Multiple ChoiceDocumento304 pagineChapter 1. Issues and Trends in Pediatric Nursing: Multiple ChoiceDENIS KAMANGUNessuna valutazione finora
- TestBank Norris Porths Essentials Pathophysiology 5e 2019Documento505 pagineTestBank Norris Porths Essentials Pathophysiology 5e 2019Cindy Perez0% (1)
- C 13Documento11 pagineC 13Jo100% (1)
- Push 3Documento2 paginePush 3Sandeep SharmaNessuna valutazione finora
- Concept MapDocumento6 pagineConcept Mapapi-499028250Nessuna valutazione finora
- Concept Map Et Al 11-04-15Documento7 pagineConcept Map Et Al 11-04-15api-353656227Nessuna valutazione finora
- Chapter 20: Postpartum Physiologic Changes Lowdermilk: Maternity & Womens Health Care, 11th EditionDocumento11 pagineChapter 20: Postpartum Physiologic Changes Lowdermilk: Maternity & Womens Health Care, 11th EditionNurse UtopiaNessuna valutazione finora
- Guide to Physical Assessment DocumentationDocumento3 pagineGuide to Physical Assessment Documentationsandaman2225Nessuna valutazione finora
- Cardiology Teaching PackageDocumento9 pagineCardiology Teaching PackageRicy SaiteNessuna valutazione finora
- BSN Reflective Journal on Postpartum Hemorrhage ScenarioDocumento2 pagineBSN Reflective Journal on Postpartum Hemorrhage ScenarioJennifer Goodlet100% (1)
- Vascularaccess 508 PDFDocumento4 pagineVascularaccess 508 PDFVina YuwandaNessuna valutazione finora
- Medical Surgical QuizDocumento12 pagineMedical Surgical QuizLyka DimayacyacNessuna valutazione finora
- Drugs Affecting The Respiratory SystemDocumento151 pagineDrugs Affecting The Respiratory SystemMajestic RavenNessuna valutazione finora
- NR 500NP WK 6 Area of Interest Power PresentationDocumento2 pagineNR 500NP WK 6 Area of Interest Power PresentationEassignmentsNessuna valutazione finora
- 351-Discussion Board 2Documento2 pagine351-Discussion Board 2api-546070989Nessuna valutazione finora
- Care PlanDocumento11 pagineCare PlanAlyssa CardinalNessuna valutazione finora
- Main drug therapy for ulcerative colitis is sulfa for one yearDocumento4 pagineMain drug therapy for ulcerative colitis is sulfa for one yearcathyNessuna valutazione finora
- Location at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Documento5 pagineLocation at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Eduard RiparipNessuna valutazione finora
- Chapter 36 - Inflammatory & Structural Heart DisordersDocumento6 pagineChapter 36 - Inflammatory & Structural Heart Disordersjosie teehNessuna valutazione finora
- Completed Concept MapDocumento4 pagineCompleted Concept Mapapi-607361848Nessuna valutazione finora
- Running Head: Scope of Practice Is State Regulated 1Documento7 pagineRunning Head: Scope of Practice Is State Regulated 1Carole MweuNessuna valutazione finora
- Bates' Visual Guide To Physical Examination Vol. 7: Head, Eyes, and EarsDocumento9 pagineBates' Visual Guide To Physical Examination Vol. 7: Head, Eyes, and EarsArlene DaroNessuna valutazione finora
- Comprehensive Nursing Assessment For Care Plan: AllergiesDocumento14 pagineComprehensive Nursing Assessment For Care Plan: AllergiesBrittany ShrewsburyNessuna valutazione finora
- Pharm Phlash PDFDocumento207 paginePharm Phlash PDFAdiShine100% (1)
- 106 Prefi Critical Care Nclex ReviewDocumento10 pagine106 Prefi Critical Care Nclex ReviewraigeneNessuna valutazione finora
- Patient Case Presentation StructureDocumento30 paginePatient Case Presentation StructureAmira HelayelNessuna valutazione finora
- How To Treat: Septic ShockDocumento6 pagineHow To Treat: Septic ShockmeeandsoeNessuna valutazione finora
- Presented By: Anjani.S.Kamal 1 Year MSC (N)Documento23 paginePresented By: Anjani.S.Kamal 1 Year MSC (N)shubham vermaNessuna valutazione finora
- Physical Examination Health AssessmentDocumento2 paginePhysical Examination Health AssessmentRosa Willis0% (1)
- Nurs324 Professional Development PlanDocumento15 pagineNurs324 Professional Development Planapi-240550685Nessuna valutazione finora
- Managing Angina: AHA Guidelines on Diagnosis and TreatmentDocumento96 pagineManaging Angina: AHA Guidelines on Diagnosis and TreatmentJaymica Laggui DacquilNessuna valutazione finora
- NURS 209-Study GuideDocumento22 pagineNURS 209-Study GuideTenzin KelsangNessuna valutazione finora
- 5P Handoff SheetDocumento1 pagina5P Handoff SheetBarry SeeboNessuna valutazione finora
- Changing Mainline IV BagDocumento5 pagineChanging Mainline IV BagLorna PaghunasanNessuna valutazione finora
- NURSING CARE OF ADULTS II: Passbooks Study GuideDa EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNessuna valutazione finora
- Vascular Responses to PathogensDa EverandVascular Responses to PathogensFelicity N.E. GavinsNessuna valutazione finora
- HEALTH EDUCATION GUIDEDocumento84 pagineHEALTH EDUCATION GUIDEJesus Mario Lopez100% (2)
- Determinants of LET Performance 1325756724Documento13 pagineDeterminants of LET Performance 1325756724Jesus Mario LopezNessuna valutazione finora
- Health Education Theories OverviewDocumento14 pagineHealth Education Theories OverviewJesus Mario LopezNessuna valutazione finora
- Health Education, Models and MethodsDocumento41 pagineHealth Education, Models and MethodsJesus Mario LopezNessuna valutazione finora
- Revised Implementing Rules and Regulations (Irr) GoverningDocumento18 pagineRevised Implementing Rules and Regulations (Irr) GoverningLj FerolinoNessuna valutazione finora
- Circulatory SystemDocumento26 pagineCirculatory SystemJesus Mario LopezNessuna valutazione finora
- Healthedu 160430181040Documento161 pagineHealthedu 160430181040Jesus Mario LopezNessuna valutazione finora
- HEALTH EDUCATION: PREPARING NURSESDocumento53 pagineHEALTH EDUCATION: PREPARING NURSESJesus Mario LopezNessuna valutazione finora
- Healthedu 160430181040Documento161 pagineHealthedu 160430181040Jesus Mario LopezNessuna valutazione finora
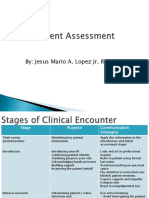
- Patient Assessment For RT'sDocumento82 paginePatient Assessment For RT'sJesus Mario LopezNessuna valutazione finora
- Airway CareDocumento68 pagineAirway CareJesus Mario LopezNessuna valutazione finora
- Rcea 00Documento59 pagineRcea 00Jesus Mario LopezNessuna valutazione finora
- Healthedu 160430181040Documento161 pagineHealthedu 160430181040Jesus Mario LopezNessuna valutazione finora
- Neonatal Lab (Assessment)Documento12 pagineNeonatal Lab (Assessment)Jesus Mario LopezNessuna valutazione finora
- Anatomy of The Renal System: By: Jesus Mario A. Lopez JR., RN, RTRPDocumento23 pagineAnatomy of The Renal System: By: Jesus Mario A. Lopez JR., RN, RTRPJesus Mario LopezNessuna valutazione finora
- Respiratory pharmacology guideDocumento45 pagineRespiratory pharmacology guideJesus Mario LopezNessuna valutazione finora
- Principles of Infection ControlDocumento35 paginePrinciples of Infection ControlJesus Mario LopezNessuna valutazione finora
- Patient Assessment For RT'sDocumento82 paginePatient Assessment For RT'sJesus Mario LopezNessuna valutazione finora
- Situation Review PDFDocumento23 pagineSituation Review PDFJesus Mario LopezNessuna valutazione finora
- Acid/Base and ABG Interpretation Made SimpleDocumento45 pagineAcid/Base and ABG Interpretation Made SimpleekadtorNessuna valutazione finora
- Writing ProposalsDocumento25 pagineWriting ProposalsSihamou AltawbaNessuna valutazione finora
- Writing ProposalsDocumento25 pagineWriting ProposalsSihamou AltawbaNessuna valutazione finora
- Sleep Workshop 3Documento71 pagineSleep Workshop 3Jesus Mario LopezNessuna valutazione finora
- Situation Review PDFDocumento23 pagineSituation Review PDFJesus Mario LopezNessuna valutazione finora
- Newer Vent ModesDocumento65 pagineNewer Vent ModesJesus Mario LopezNessuna valutazione finora
- Pathology ReviewDocumento40 paginePathology ReviewSam Fliker100% (1)
- SBTDocumento1 paginaSBTJesus Mario LopezNessuna valutazione finora
- Respiratory PharmacologyDocumento41 pagineRespiratory PharmacologyJesus Mario Lopez100% (1)
- Respiratory Ana PhysioDocumento93 pagineRespiratory Ana PhysioJesus Mario LopezNessuna valutazione finora
- Principles of Infection ControlDocumento35 paginePrinciples of Infection ControlJesus Mario LopezNessuna valutazione finora
- HAADStatisticsEng2013 PDFDocumento91 pagineHAADStatisticsEng2013 PDFHitesh MotwaniiNessuna valutazione finora
- Influence of Anthropometric Parameters On Aerobic Capacity Among DancersDocumento7 pagineInfluence of Anthropometric Parameters On Aerobic Capacity Among DancersAnonymous izrFWiQNessuna valutazione finora
- Drug Study - MidazolamDocumento2 pagineDrug Study - MidazolamKian HerreraNessuna valutazione finora
- VoltarenTab PDFDocumento6 pagineVoltarenTab PDFhmarcalNessuna valutazione finora
- Pharmacovigilance Classification & CodingDocumento42 paginePharmacovigilance Classification & Codingrakesh meher0% (1)
- 1 PBDocumento21 pagine1 PBDewi Puspita SariNessuna valutazione finora
- Tracheostomy Care With ChecklistDocumento5 pagineTracheostomy Care With ChecklistHollan GaliciaNessuna valutazione finora
- 4 Levels of Perio DZDocumento2 pagine4 Levels of Perio DZKIH 20162017Nessuna valutazione finora
- 1413272524world10 15 14 PDFDocumento38 pagine1413272524world10 15 14 PDFCoolerAdsNessuna valutazione finora
- Jobs Safety Analysis for Radiography WorkDocumento4 pagineJobs Safety Analysis for Radiography WorkGan KusumaNessuna valutazione finora
- Multidrug Resistant Gram Negative BacteriaDocumento6 pagineMultidrug Resistant Gram Negative BacteriaAniAliciaOrtizCastleNessuna valutazione finora
- Unit 2 Chapter 11 AnswersDocumento7 pagineUnit 2 Chapter 11 AnswersLeeanaNessuna valutazione finora
- Principles of Pharmocodynamics 2 (Autosaved)Documento35 paginePrinciples of Pharmocodynamics 2 (Autosaved)dv94gw9zd8100% (1)
- General Survey TECHNIQUE Actual Findings Normal Findings AnalysisDocumento21 pagineGeneral Survey TECHNIQUE Actual Findings Normal Findings AnalysisJerry Joseph B. AbordoNessuna valutazione finora
- Toxic Metabolic Encephalopathy John W. Melton, M.DDocumento17 pagineToxic Metabolic Encephalopathy John W. Melton, M.DabdalkhalidNessuna valutazione finora
- Seminar on Concepts and Foundations of RehabilitationDocumento13 pagineSeminar on Concepts and Foundations of Rehabilitationamitesh_mpthNessuna valutazione finora
- Revised Market Potential Estimates for Biopure's Hemopure Based on Competitive LandscapeDocumento4 pagineRevised Market Potential Estimates for Biopure's Hemopure Based on Competitive Landscapeargand_xw9097Nessuna valutazione finora
- Presentation - Oral Controlled Release DrugDocumento38 paginePresentation - Oral Controlled Release DrugMrValentynNessuna valutazione finora
- Quick Guide to Bandaging TechniquesDocumento4 pagineQuick Guide to Bandaging TechniquesTheodore GonzaloNessuna valutazione finora
- Past PE Papers Viva TopicsDocumento29 paginePast PE Papers Viva TopicsLouis MasonNessuna valutazione finora
- 74 Manila Pest Control Vs WCCDocumento4 pagine74 Manila Pest Control Vs WCCharryNessuna valutazione finora
- Biochemistry For Anesthesiologists and IntensivistsDocumento11 pagineBiochemistry For Anesthesiologists and IntensivistsAndi tenri sanda datuNessuna valutazione finora
- 2014 Windsor University Commencement Ceremony PROOFDocumento28 pagine2014 Windsor University Commencement Ceremony PROOFKeidren LewiNessuna valutazione finora
- TH THDocumento11 pagineTH THFista Divi AmesiaNessuna valutazione finora
- Angels Bridging Angels Bridging Angels Bridging Angels Bridging Gaps Gaps Gaps GapsDocumento13 pagineAngels Bridging Angels Bridging Angels Bridging Angels Bridging Gaps Gaps Gaps Gapsapi-251664135Nessuna valutazione finora
- Functional Foods and Nutraceuticals-ModeDocumento18 pagineFunctional Foods and Nutraceuticals-ModediahNessuna valutazione finora
- Rosemont Health Center Rev01Documento7 pagineRosemont Health Center Rev01Amit VishwakarmaNessuna valutazione finora
- Safe AnalgesicsDocumento3 pagineSafe AnalgesicsJohn SolisNessuna valutazione finora
- BurosumabDocumento8 pagineBurosumabutamiprakosoNessuna valutazione finora
- Effects of Boiling Time On Mineral and Vitamin C Content of Three Varieties of Hibiscus Sabdriffa Drink in NigeriaDocumento6 pagineEffects of Boiling Time On Mineral and Vitamin C Content of Three Varieties of Hibiscus Sabdriffa Drink in NigeriariniyuliasamosirNessuna valutazione finora